Mammography has been the primary mode of breast cancer screening and diagnosis for more than 20 years, and it has saved many lives. But the medical community continues to encounter women for whom screening mammography appears to have fallen short.
Between 1996 and 2000, white women in the U.S. had, on average, 140.8 incidences of breast cancer per 100,000, with 27.2 women dying from the disease, according to a recent Report to the Nation produced by the American Cancer Society (ACS), the Centers for Disease Control (CDC), the National Cancer Institute (NCI), and the North American Association of Central Cancer Registries (NAACCR).
During the same time period, African-American women had 121.7 incidences and 35.9 deaths per 100,000 women; Hispanic women had 89.8 incidences and 17.9 deaths; Asian/Pacific Islander women had 97.1 incidences and 12.5 deaths; and American Indian/Alaskan native women had 58.0 incidences and 14.9 deaths.
The fact that white women in the U.S. have a higher incidence of breast cancer than other racial or ethnic groups is likely to reflect a combination of several factors, according to Dr. Michael Thun, head of the ACS epidemiology research group. These include more frequent screening mammography (which finds tumors earlier), past reproductive patterns (fewer children and later age at first birth), greater alcohol consumption, and greater use of hormone replacement therapy. But why do women in other racial groups -- in particular, African-American women -- have more advanced-stage cancer when they are diagnosed?
"Other racial and ethnic groups have a higher proportion of tumors diagnosed at advanced stage with large tumor size. This is thought to be attributable largely to socioeconomic factors, such as access to high-quality mammography and appropriate treatment. But other, unidentified factors may influence breast cancer outcomes as well," Thun said.
One theory is that cultural norms or beliefs affect women’s compliance with regular screening mammograms. Another is that socioeconomic differences create unequal access to healthcare. Still another hypothesis is that there may be physical differences between women of different races that affect mammography’s efficacy and/or sensitivity. It’s likely that the answer to the question of why women of different races experience different breast cancer outcomes is a complex matrix of all the above factors, in addition to others that remain unclear.
Cultural beliefs, cancer outcomes
Women’s advocacy groups and healthcare workers have become increasingly aware that women respond to culture-specific education about the necessity of regular mammograms. In a study published in Cancer, Dr. Shin-Ping Tu and colleagues examined whether cultural norms within the Chinese-American community may influence compliance with mammography protocols. They found that Chinese-American women were most likely to have a mammogram if their primary care doctor told them to -- and if that doctor was a female Chinese speaker.
Tu also found that the cultural convictions of a Chinese-American woman weren’t necessarily a negative factor in shaping her attitudes toward breast cancer screening. Rather, it depended on her cultural framework: Those who felt that disease was caused by imbalances of yin and yang were more resistant to screening, but women who felt that disease could be caused by poor qi and blood circulation were more inclined to screening, according to the study (Cancer, March 1, 2003, Vol. 97:5, pp.1293-1302).
Although many clinicians agree that access to standardized screening mammography and follow-up has improved for women across racial and ethnic lines, access and quality of care remain crucial issues. In a study in the Archives of Internal Medicine, Dr. Christopher Li and colleagues at the Fred Hutchinson Cancer Research Center in Seattle found that breast cancer treatment varied by race.
They presented data from about 125,000 U.S. women from different races and ethnic groups, who were diagnosed with breast cancer between January 1992 and December 1998. African-Americans, American Indians, Hawaiians, Vietnamese, Mexicans, South and Central Americans, and Puerto Ricans were 20% to 200% more likely to die from breast cancer compared to white women; these women, plus Indians and Pakistanis, were also 1.4 to 3.6 times more likely to receive a diagnosis of advanced-stage cancer than white women (Archives of Internal Medicine, Jan. 13, 2003; Vol.163:1, pp. 49-56).
"Differences in breast cancer stage, treatment, and survival by race and/or ethnicity are attenuated when socioeconomic factors are controlled for," Li said. "Improving access to screening and providing culturally appropriate care is crucial for addressing these disparities."
In another study, Dr. Lisa Baron and colleagues at the Medical University of South Carolina in Charleston examined whether women of different races received a clinical breast exam (CBE) before screening mammograms.
They found that out of 1,017 women undergoing screening, 50.2% reported having had a CBE within the previous 12 months. Of the 364 women of color, only 38.5% reported having undergone CBE in this time period before screening mammography, while 57.4% of the 638 white women included in the study had CBE (Radiology, August 2002, Vol. 224:2, pp. 555-559).
"Physicians referring women for screening mammography need to adhere to national guidelines by performing annual CBE," the authors wrote. "In particular, physicians need to focus on performing CBE in nonwhite, less educated, and older women. Radiologists interpreting screening mammograms should be aware that many women have not been screened with CBE and hence may not be asymptomatic."
Physical differences and mammographic efficacy
Age-adjusted breast cancer mortality rates in the U.S. among white and African-American women have been diverging for the past 20 years. To find out why, Dr. Ismail Jatoi and colleagues at the Uniformed Services University of the Health Sciences in Bethesda, MD, examined medical records of all women diagnosed with primary breast cancer between 1980 and 1999 in the U.S. Department of Defense (Cancer, September 2003, Vol. 98:5, pp. 894-899).
Jatoi and colleagues wanted to explore whether there would be other factors that contribute to African-American women’s higher mortality rate from breast cancer besides that of unequal access. The final dataset included 23,612 women. Within that group, the researchers found that the survival of African-American women, compared to that of white women, still manifested in an increasing "hazard ratio" during that time period, with a greater risk of death for the African-American women.
Jatoi concluded that inequalities in access to healthcare -- in this case mammography -- is not the sole factor for widening racial disparities in outcomes for women with breast cancer.
"What this study demonstrates is that breast cancer survival rates among African-American and Caucasian women are diverging in the Department of Defense healthcare system," Jatoi wrote in an e-mail to AuntMinnie.com. "Since the U.S. Department of Defense system is an equal-access healthcare system, the fact that survival rates among Caucasian and African-American women (continue to diverge) suggests that access to healthcare is not solely responsible for the widening racial disparities in breast cancer outcomes between these two groups of women."
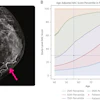
Radiologists and technologists have long known that breast density affects mammography’s efficacy: The technology doesn’t perform as well on women with dense breast tissue. It is for this reason, in part, that younger women aren’t regularly screened, as breast tissue tends to become less dense as women age. It’s also known that a woman’s weight and body mass index (BMI) affect the composition of her breast tissue, with women in the higher BMI quartiles having less-dense breast tissue than women in the lower quartiles. But can these factors be extrapolated to explain disparities in breast cancer outcomes between women of different racial groups?
Dr. Kevin Hughes and colleagues at Massachusetts General Hospital in Boston used mammograms from 769 women to explore whether there is a difference in breast tissue density among African-American, Caucasian, and Latina women. Women who were scheduled for biopsy due to abnormal mammography results were eligible for the study; reasons or ineligibility included breast implants or weighing more than 300 pounds (CancerM, August 2003; Vol. 98:3. pp. 590-596).
The MGH group posited that the sensitivity of mammography as a screening tool is inversely proportional to the breast tissue density of the women being screened. Breast tissue density decreases as women age, and is also affected by weight and BMI.
In the study group, the percentage of women (mean age 55 years) who were both overweight and obese (BMI equal to or greater than 25 kg/m2) was 79% for African-American women, 57% for Caucasians, and 69% for Latinas.
Because African-American women seem to bear a heavier breast cancer mortality burden, the researchers’ hypothesis had been that they might have denser breast tissue, which would affect mammography’s sensitivity and therefore breast cancer outcomes. However, they discovered that the African-American women actually had the lowest mean breast density as compared to the Caucasian and Latina women. If breast density were the only factor that determined mammography’s efficacy, this study would seem to underscore mammography's importance as an effective breast cancer screening modality for African-American women.
That these women have a higher breast cancer mortality rate points to other factors, according to the study, such as biologic characteristics of tumors found in African-American women, which tend to be characterized by a younger age of diagnosis, larger size, and less-favorable histology. These factors would suggest that the traditional protocol for screening mammography -- starting at age 40 and continuing at one-year intervals between mammograms -- might be less effective for African-American women.
Hughes’s study raises the question of whether there are particular physical differences between women across racial or ethnic lines that should be considered for screening mammography purposes. Not only does breast density affect mammography’s efficacy, but breast size does as well.
Mosaic imaging, which is required when the patient’s breast is bigger than the detector, can decrease efficiency, as well as increasing the dose, scatter, and imaging time, which can make the detection of small lesions more difficult. In fact, there is some discussion in the clinical community about how facilities can best match detector size -- particularly for mobile, digital units -- to their screening population, according to a recent AuntMinnie article.
In any case, the disparity in breast cancer outcomes between women of different races has been established, according to Hughes. The question remains as to why the disparity exists.
"Once we identify the factors that contribute to this problem, we can begin to address them," he said. "But the danger is that by jumping to conclusions, we’ll miss something crucial."
By Kate Madden YeeAuntMinnie.com contributing writer
October 10, 2003
Related Reading
Calif. Asians, Latinos miss cancer screening-study, September 18, 2003
Diverse Los Angeles population gives cancer clues, August 22, 2003
Mammographic breast density lower in African American women, August 18, 2003
Statistics suggest strategies for cancer reduction among Hispanics, August 11, 2003
Racial inequities in healthcare not only factor influencing breast cancer survival, July 29, 2003
Chinese women respond best to doctors' breast cancer screening advice, February 19, 2003
Non-whites in U.S. at greater risk for advanced breast cancer, January 14, 2003
Copyright © 2003 AuntMinnie.com