Ann Surg Oncol 1999 Jul-Aug;6(5):450-4 (Comment in: Ann Surg Oncol. 1999 Jul-Aug;6(5):418-9)
Intradermal radiocolloid and intraparenchymal blue dye injection optimize
sentinel node identification in breast cancer patients.
Linehan DC, Hill AD, Akhurst T, Yeung H, Yeh SD, Tran KN, Borgen PI, Cody HS
3rd.
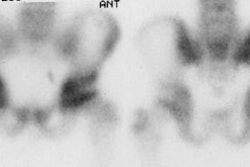
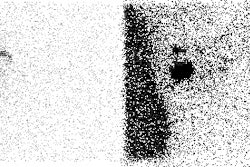
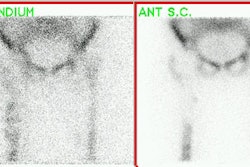
BACKGROUND: Radiotracer and blue dye mapping of sentinel lymph nodes (SLN) have
been advocated as accurate methods to stage the clinically negative axilla in
breast cancer patients. The technical aspects of SLN biopsy are not fully
characterized. In this study we compare the results of intraparenchymal (IP) and
intradermal (ID) injection of Tc-99m sulfur colloid, to establish an optimal
method for SLN localization. METHODS: 200 consecutive patients had SLN biopsy
performed by a single surgeon. Of these, 100 (Group I) had IP injection and 100
(Group II) had ID injection of Tc-99m sulfur colloid. All patients had IP
injection of blue dye as well. Endpoints included (1) successful SLN
localization by lymphoscintigraphy, (2) successful SLN localization at surgery,
and (3) blue dye-isotope concordance (uptake of dye and isotope by the same SLN).
RESULTS: Isotope SLN localization was successful in 78% of Group I and 97% of
group II patients (P < .001). When isotope was combined with blue dye, SLN
were found in 92% of group I and 100% of Group II (P < .01). In cases where
both dye and isotope were found in the axilla, dye mapped the same SLN as
radiotracer in 97% of Group I and 95% of Group II patients. CONCLUSIONS: The
dermal and parenchymal lymphatics of the breast drain to the same SLN in most
patients. Because ID injection is easier to perform and more effective, this
technique may simplify and optimize SLN localization.