A review paper in the October issue of the American Journal of Roentgenology describes some of the errors that occur in chest radiography exams in children, with the goal of educating radiology professionals about the types of pathologies and disorders -- both frequent and infrequent -- they can encounter in kids.
The team led by Dr. Sarah Menashe of Seattle Children's Hospital believes that a systematic approach to image interpretation -- with an awareness of common errors and their causes -- can help both general and pediatric radiologists when interpreting images (AJR, Vol. 207:4, pp. 903-911). The authors walk readers through anatomical regions of the chest such as the mediastinum, lungs and pleura, and bones, providing a series of case studies with teaching points that represent the difficulties that can be encountered in each region.
AJR is offering the study on an open-access basis.
Mediastinum
Even the normal mediastinum can have a variable appearance on radiographs of children, depending on factors such as age, developmental stage, and health status, as well as anatomical variations of the thymus. While cross-sectional modalities such as CT and MRI are available, they are rarely used as first-line tools.
Teaching points for radiographic imaging of the pediatric mediastinum include the following:
- The thymic gland appears as a lobulated and occasionally triangular-shaped soft-tissue density with a degree of transparency on chest radiographs. The transparency allows visualization of underlying lung vessels.
- On all radiographs of the pediatric chest, radiologists should assess the caliber and position of the trachea and the laterality of the aortic arch. These can provide the first clues of the presence of a vascular anomaly.
- Thoracic paraspinal lines should be thin on all projections; if a posterior mediastinal mass is found in a young child, it should be considered a neuroblastoma until proved otherwise.
- "Vanishing heart" refers to cases of abnormal lucency over the heart shadow over time; this is a sign of posterior pneumomediastinum.
Lungs and pleura
Proper visualization of the lungs on pediatric radiography is subject to correct technique and patient cooperation, both of which can be difficult to obtain in pediatric imaging. True findings can be obscured by factors such as tube angle, patient rotation, patient breathing, and tube voltage settings, and false findings can be created when not properly controlled. Lung ultrasound is sometimes useful but has issues of its own; contrast-enhanced CT is occasionally warranted.
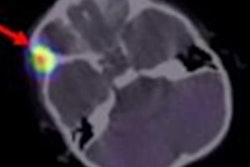
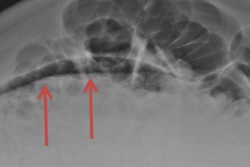
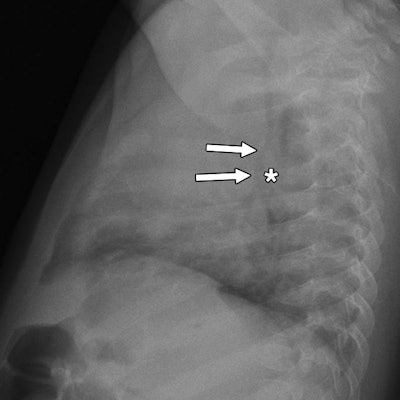
 Images are of a 4-month-old boy with breathing difficulty. Frontal (left) and lateral (right) chest radiographs show diffuse narrowing of intrathoracic trachea (arrows, left) and subtle anterior displacement of inferior trachea (arrows, right) by soft-tissue density (asterisk, right) interposed between trachea and esophagus. These findings were not described on the report. Images courtesy of AJR.
Images are of a 4-month-old boy with breathing difficulty. Frontal (left) and lateral (right) chest radiographs show diffuse narrowing of intrathoracic trachea (arrows, left) and subtle anterior displacement of inferior trachea (arrows, right) by soft-tissue density (asterisk, right) interposed between trachea and esophagus. These findings were not described on the report. Images courtesy of AJR. 3D reformat from CT performed two weeks later, showing left pulmonary artery sling and diffusely narrowed trachea (arrows) secondary to complete tracheal rings, which are commonly associated with this type of vascular ring.
3D reformat from CT performed two weeks later, showing left pulmonary artery sling and diffusely narrowed trachea (arrows) secondary to complete tracheal rings, which are commonly associated with this type of vascular ring.The authors noted the following important points:
- Instances of new lucency found within densely consolidated lung should create suspicion of pulmonary necrosis, which can be confirmed with cross-sectional imaging.
- Lung masses detected prenatally should be followed postnatally with radiography and eventually with contrast CT.
Bones
Although neonatal radiographs are usually acquired for evaluating respiratory and gastrointestinal systems, clinically useful information can often be found by evaluating osseous structures. Clues to underlying pathologies such as metabolic bone disease, congenital or neonatal infection, or nonaccidental trauma can be discovered in sometimes subtle bony findings of osteopenia, fractures, or periosteal reaction. Tips include the following:
- Correct diagnosis and patient management depend on careful attention to and documentation of bony findings, as well as correlation with patient history and communication with the clinical team.
- Signs of cortical thinning and associated fractures in premature infants can indicate bony demineralization and suggest underlying metabolic bone disease related to prematurity.
- Periostitis in the periosteal membrane covering cortical bone can occur in the first six months, usually at about 12 weeks of age. It's important to evaluate the pattern and extent of bony involvement, and to correlate it with clinical and biochemical markers to determine a diagnosis.
- While there are many disorders that can affect the appearance of the skeletal system, it's important to be able to recognize some of the more common disorders. Bony abnormalities on radiography can serve up key information needed to diagnose conditions such as skeletal dysplasia or syndrome.
The authors concluded by noting that in the age of as low as reasonably achievable (ALARA) imaging, additional radiography projections or referral to cross-sectional imaging is not always appropriate.
"Having a thorough understanding of normal pediatric anatomy and developmental changes along with a good command of the entities unique to children is essential for the pediatric and general radiologist to avoid significant interpretive errors," said paper co-author Dr. A. Luana Stanescu of Seattle Children's Hospital in a prepared statement. "Errors in interpretation may lead to inappropriate further imaging, incurring additional radiation exposure and cost, as well as psychologic effects on the patients and their families."