CHICAGO - Absorbed organ doses are very close to size-specific dose estimates (SSDE) in CT exams of the abdomen and pelvis, confirming the validity of radiology's new and more accurate dose measurement technique, according to a study presented at the RSNA meeting.
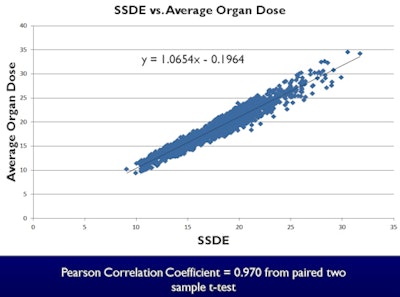
Researchers from the Henry Ford Health System in Detroit found a linear relationship between SSDE and mean absorbed organ doses, measuring a slope of 1.05 and a Pearson correlation coefficient of 0.97.
"SSDE is indeed a reliable indicator of organ doses in the abdomen and pelvis when the organ of interest is fully covered in the exam," concluded Mark Supanich, PhD, in his Wednesday presentation. "SSDE offers a rapid, straightforward method to estimate organ doses without the need for Monte Carlo simulations."
 |
| A linear relationship between 0.75 and 1.33 was observed for individual organ doses and SSDE. Image courtesy of Mark Supanich, PhD. |
SSDE, a metric that accounts for patient size, scan length, and tissue attenuation, was introduced last year by the American Association of Physics in Medicine (AAPM) Report 204 as an indicator of absorbed organ doses, Supanich explained. That paper presented a set of conversion factors (called F-factors) to take clinicians from CT dose index volume (CTDIvol) to a better and more accurate estimation of patient dose. Since last year, at least a dozen studies have been published describing the use of SSDE in clinical populations.
The current study was designed to obtain further validation of SSDE as a measure of patient dose.
"In this case, we were looking at using the effective diameter to calculate the F-factor from the CT image -- so using the CT image to determine the effective diameter [based on a water phantom calculation] of the patient, and using that to determine the F-factor," Supanich said. "And we also looked at the SSDE calculated by that method to determine the average organ dose in clinical studies done at our institution."
The researchers began with 1,250 noncontrast CT scans covering the abdomen and pelvis, which were retrospectively analyzed for the study. Images were acquired over a 10-month period using both axial and longitudinal tube-current modulation on seven 64-detector-row scanners (5 from Philips Healthcare; 2 from GE Healthcare). The effective diameter, the F-factors, and the organ dose estimates were all acquired using a commercially available software package (eXposure, Radimetrics). The researchers calculated effective diameter from the midscan CT image, using a water cylinder with a diameter equivalent to the total attenuation of that CT image.
Monte Carlo simulations were used for organ dose calculations. The eXposure software uses the Cristy/Eckerman set for Monte Carlo simulation for adults from a male (28.3 cm) and a female (25 cm) anthropomorphic phantom. Only patients with measurements with calculated effective diameters within 2 cm of the phantom sizes were included in the study; otherwise, "we could have included a lot more than 1,200 studies," Supanich said.
"The reason we did this is we saw that the further you moved away from the diameter of the phantom, the accuracy of the organ dose calculations just wasn't there" -- it deteriorated significantly as the phantom and patient sizes diverged, he explained.
Organ dose estimates were calculated and averaged for the gallbladder, kidneys, liver, spleen, and stomach, in addition to the cervix in female patients.
The results showed that SSDE values ranged from 10 to 32 mGy over the study population, and CTDIvol ranged from 6.4 to 23.8 mGy. Effective diameters ranged from 23.5 to 30.3 cm, which corresponded to an F-factor from the AAPM 204 report of just over 1.5. F-factors ranged from 1.2 to 1.55.
Results comparing linear fit between SSDE and calculated average organ dose
|
"There was an excellent -- pretty much 1:1 -- relationship between SSDE and the average absorbed organ dose, as we would expect given the data that went into the AAPM 204 report," he said. "Some of the organs, probably due to their position within the patient, do have slightly different fits to the SSDE, but overall the correlation ... was fairly strong." Results in the uterus showed a factor of 1.8 increase in the absorbed dose compared to SSDE.
SSDE is a reliable indicator of organ dose when the exam covers the entire organ, Supanich said, and it offers a rapid, straightforward method of estimating organ doses without need of Monte Carlo simulations. Individual organ doses may be able to be simulated using SSDE, he concluded.
Study limitations included use of SSDE only from the central CT slice, and the fact that average CTDIvol was used to perform the Monte Carlo calculations.