A software-based technique aimed at deriving CT-based blood flow data without invasive procedures showed similar accuracy to invasive fractional flow reserve (FFR) for determining the significance of coronary stenosis, according to a new report in the American Journal of Cardiology.
In the first published study to use the investigational software to perform fast-flow computation of coronary blood flow from coronary CT angiography (CCTA) images, researchers compared the results to invasive fractional flow reserve. They found a sensitivity of 85% per vessel and 94% per patient, with high positive and negative predictive values (Am J Cardiol, August 11, 2014).
The software also outperformed CCTA alone for the detection of flow-limiting stenosis. And unlike another software-based FFR-CT method that has been validated in larger trials, the new technique doesn't require shipping image data to an offsite lab for processing.
"What this software does is add much-needed specificity that helps you determine whether a lesion means something in terms of limiting blood flow to the myocardium," said study co-author Dr. U. Joseph Schoepf, director of cardiovascular imaging at the Medical University of South Carolina (MUSC), in an interview.
Alternatives to invasive FFR
Conventional FFR assesses blood flow via catheterization with a pressure wire that measures actual blood flow through a coronary artery.
But while invasive FFR improves the detection of obstructive coronary artery disease, it is expensive and time-consuming. To a far lesser extent, the drawbacks are similar for another CT-based FFR application called HeartFlow, which is performed after the radiologist transfers a CT dataset to an external lab for computation, waiting one to four hours for its return.
The retrospective study by Schoepf and colleagues investigated the diagnostic performance of the new algorithm (cFFR, version 1.4, Siemens Healthcare), developed for evaluating hemodynamically indeterminate coronary lesions that were confirmed by invasive FFR. Unlike HeartFlow, users of cFFR can generate FFR data onsite.
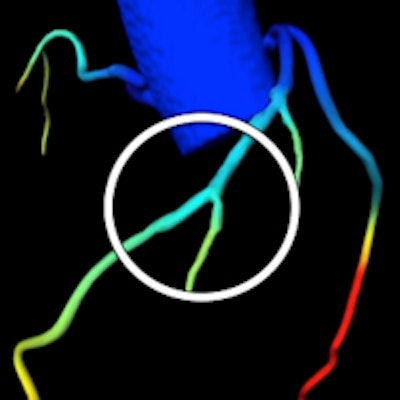
 A calcified stenosis in the middle left anterior descending (LAD) artery seen on CCTA (left) was suspected to be significant. However, CT-based FFR demonstrated the absence of lesion-specific ischemia by the color-coded coronary artery tree model (right), which was confirmed by subsequent coronary catheter angiography with invasive FFR derivation. Image courtesy of Dr. Matthias Renker and Dr. U. Joseph Schoepf.
A calcified stenosis in the middle left anterior descending (LAD) artery seen on CCTA (left) was suspected to be significant. However, CT-based FFR demonstrated the absence of lesion-specific ischemia by the color-coded coronary artery tree model (right), which was confirmed by subsequent coronary catheter angiography with invasive FFR derivation. Image courtesy of Dr. Matthias Renker and Dr. U. Joseph Schoepf.The researchers assessed the cFFR software's performance on 67 coronary lesions in 53 patients with suspected or known coronary artery disease who had undergone CCTA on a dual-source CT scanner (Somatom Flash, Siemens) between 2008 and 2014.
Patients also underwent conventional invasive coronary angiography, in which luminal stenosis was graded visually by an experienced interventional cardiologist. Invasive FFR was also conducted at the time of coronary angiography if the stenosis was suspected of causing ischemia, wrote the authors from MUSC, as well as the Kerckhoff Heart and Thorax Center in Bad Nauheim, Germany; Capital Medical University in Beijing; and Heidelberg University in Mannheim, Germany.
An experienced reader looked at all CCTA studies, visually determining the luminal diameter stenosis of each lesion of interest using transverse CT sections and curved multiplanar reformats on a dedicated workstation (syngo.via, Siemens). Datasets were also rated qualitatively on a five-point scale with 5 meaning "excellent."
New algorithm gauges blood flow
The cFFR software is based on principles of computational fluid dynamics and simulates coronary blood flow from the 3D boundary conditions for a hyperemic state. Once the software generated a 3D mesh of the coronary artery tree, an experienced reader blinded to angiography and invasive FFR results either accepted, rejected, or corrected the luminal contours proposed by the software, the authors explained.
Boundary conditions were represented by cardiac and coronary microcirculatory models, which integrated resting-state conditions including systolic and diastolic blood pressures, heart rate, and left ventricular mass. They were then modified to incorporate the effect of maximal hyperemia, or increased blood flow to an area, by simulating a drop in microvascular resistance, as if they had been induced by pharmacologic stressor agents. The researchers tried to apply the coronary flow model at the same position as invasive FFR, which served as the reference standard for the comparisons.
Stenosis was defined as FFR less than 0.80 on pressure guidewire-based FFR (stenoses at CT are considered significant with 50% or greater luminal narrowing).
In the 53 patients (67 vessels), the cFFR algorithm had a sensitivity of 85% per lesion and 94% per patient, with specificity of 85% and 84%, respectively. Also, the software performed better than CCTA alone: The area under the receiver operator characteristics curve (AUC) was significantly higher for CT-based FFR (0.92) than standard CCTA (0.72, p = 0.00049). There was a similar trend, though it was not statistically significant, for the per-patient analysis (AUC of 0.91 for FFR-CT versus 0.78 for CCTA alone).
| cFFR vs. CCTA for coronary artery stenosis | ||||
| Measure | Per lesion | Per patient | ||
| cFFR software | CCTA | cFFR software | CCTA | |
| Sensitivity | 85% | 90% | 94% | 94% |
| Specificity | 85% | 34% | 84% | 32% |
| Positive predictive value (PPV) | 71% | 37% | 71% | 98% |
| Negative predictive value (NPV) | 93% | 89% | 97% | 32% |
The mean total time required to perform studies with the cFFR software was 37.5 ± 13.8 minutes, compared with one to four hours for the HeartFlow technique. The results for cFFR seem comparable those reported for FFR in the HeartFlow system trial, Schoepf said. Both CT-based FFR techniques are doing essentially the same job, he said: determining lesion-specific ischemia in a noninvasive manner.
Accuracy of the two methods appears similar as well, and if you look at the results carefully, cFFR seems to be even a few percentage points higher, according to Schoepf.
"So it's in the same league, and at least for the preliminary experience performs a little bit better," he said.
No software tool is going to be perfect, but invasive tools like invasive angiography aren't perfect either, Schoepf said. And FFR-CT is already easier and more straightforward than noninvasive alternatives such as SPECT myocardial perfusion imaging (MPI) and perfusion CT, which he has championed for other indications.
Still, the existing HeartFlow software has been validated in trials of many more patients, as will be needed for the cFFR software if it is to receive U.S. Food and Drug Administration (FDA) clearance. Meanwhile, HeartFlow is still waiting for its 510(k) to be cleared.
"But if you look at the data that's there on fluid dynamic modeling of CT datasets, it's showing basically what people want it to do: improve specificity for determining lesion-specific ischemia," Schoepf said. "It's been shown that patients benefit from management decisions vis-à-vis intervention that are driven by hemodynamic relevance like in lesion-specific ischemia. That's the goal, and with this software tool I think we can provide those answers substantially faster."

















