Radiation dose for whole-body pediatric PET/CT exams can be cut in half with new low-dose protocols customized to the weight of children, according to research published in the October issue of the Journal of Nuclear Medicine.
PET/CT has demonstrated its utility in adult medical imaging and is increasingly being used in pediatric applications. However, previous research has demonstrated that using adult-based protocols on children results in unnecessary radiation dose, and recent campaigns such as the Image Gently initiative are raising awareness about the need to "child-size" imaging parameters.
That was the goal of a research team from Seattle Children's Hospital and the University of Washington: The group developed a set of whole-body PET/CT acquisition parameters that try to strike a balance between image quality and radiation risk by customizing scanner acquisition parameters based on patient weight.
The authors believe that the lower settings can reduce radiation dose by at least half compared to conventional PET/CT exams. And this, in turn, would dramatically lower the risk that a pediatric patient might develop cancer later in life from a PET/CT study, according to lead author Adam Alessio, Ph.D., a research assistant professor of radiology at the University of Washington School of Medicine in Seattle (JNM, 2009, Vol. 50:10, pp. 1570-1577).
Color-coded categories
The authors used the Broselow-Luten color-coded weight scale originally developed for emergency pediatrics to create 11 weight-based categories for PET/CT exams. For each category, the authors developed protocols to vary the amount of injected FDG activity and length of PET acquisition times. They also developed weight-based tube-current protocols for the CT component of the exams.
For PET studies, the system calls for varying the level of injected FDG activity from 37 MBq for the smallest patients (category pink, weight range 6-7 kg) to 252 MBq for the largest pediatric patients (category black, weight range 40.5-55 kg). This compares to 330 MBq for small adults (55-70 kg) and 370 MBq for large adults (heavier than 70 kg).
Image acquisition times were also varied, from three minutes per field-of-view (FOV) for the smallest patients to five minutes per FOV for larger children and adults.
The researchers also developed protocols for use in CT attenuation correction and anatomic correlation with PET findings (they recommended that their protocols not be used for diagnostic CT studies). All patients were scanned with a tube voltage of 120 kVp, pitch of 0.98:1, rotation speed of 0.5 seconds, body bow-tie filter, and reconstructed slice thickness of 2.5 mm. The maximum CT current was varied for each category, from 10 mAs for patients in the pink category to 30 mAs for the black category. The largest adult patients typically are scanned at 40 mAs.
Pediatric whole-body PET/CT protocols highlighting acquisition settings varied for each weight category
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Table courtesy of the Journal of Nuclear Medicine. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The team's previous research suggested that changing the CT scanner's tube voltage would only produce modest dose savings for different patients, so the researchers decided to scan all patients with a tube voltage of 120 kVp and, instead, vary the tube current to achieve significant dose reductions. The researchers also recommend using automatic tube current modulation, but they didn't address automatic exposure control in their study because it can be highly vendor-specific.
Image quality and dose reduction
As of the study's publication date, Alessio and colleagues said that the technique had been used to image 140 patients representative of all weight categories, with all exams performed using a Discovery VCT PET/CT scanner (GE Healthcare, Chalfont St. Giles, U.K.). Nuclear medicine physicians who have reviewed the studies reported that all 140 CT exams were acceptable to localize PET activity to anatomy, according to the authors.
 |
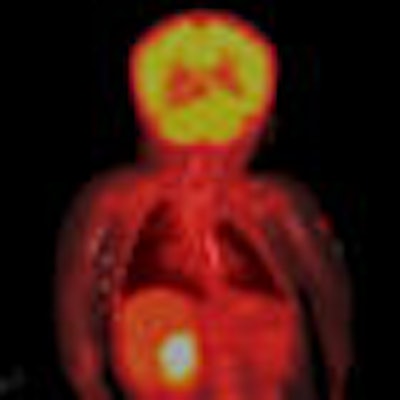
| Coronal view of CT (A), PET (B), and overlaid PET/CT image (C) of 6-kg 4-month-old. CT was performed with 120 kVp and 10 mAs, leading to image with acceptable anatomic detail. PET was performed with 37 MBq (1 mCi) of injected fluorine-18 FDG for three minutes/bed position. Image courtesy of SNM. |
To estimate radiation dose, the authors used simulation-derived dosimetry estimates, interpolating the estimates to specific categories based on weight for PET and age for CT using standard growth charts.
Young patients saw a bigger dose reduction, an important finding as they are more susceptible to radiation-induced adverse effects. For a 7-kg patient, the authors estimated that radiation dose with the new protocols would be 20% of that of a normal PET/CT exam with 120 mAs and 120 kVp CT settings. For a 70-kg patient, the dose delivered would be 50% of a conventional study.
What does that translate into in terms of cancer risk? Alessio and colleagues estimated that the risk of cancer incidence in a pediatric patient's lifetime from a single PET/CT exam using one of the new protocols is approximately 38 in 10,000, and the corresponding risk of mortality from cancer is approximately 15 in 10,000. This represents a threefold reduction in cancer risk compared to an exam conducted without varying the CT parameters according to patient weight, the authors estimated.
"The risks from PET/CT are generally far outweighed by the benefit of this procedure when used appropriately," the authors concluded. "Furthermore, pediatric PET/CT is commonly used to diagnose, stage, and monitor already-present cancer, so there is a clearly favorable benefit-to-risk ratio. It is important, however, that the imaging community is aware of the relative amount of additional risk to patients from these imaging procedures."
By Cynthia E. Keen
AuntMinnie.com staff writer
October 1, 2009
Related Reading
Radiation dose and cancer risk in pediatric CTA exams, August 21, 2009
Web site educates patients about radiation dose, July 2, 2009
Dose can be reduced by 75% in pediatric chest CT exams, June 18, 2009
Color coded CT protocols help reduce pediatric radiation dose, June 4, 2009
SPR group tackles radiation dose in pediatric nuclear medicine, May 22, 2009
Copyright © 2009 AuntMinnie.com

















