Positron emission mammography (PEM) is branching out from breast imaging, as researchers at Johns Hopkins University have used the modality with preliminary success to view osteoarthritis in patients' hand joints.
A new study, led by Dr. Joyce Mhlanga, a nuclear medicine resident in Johns Hopkins Hospital's division of radiology and radiological services, found a strong correlation between PEM and radiographic total joint scores in symptomatic osteoarthritis patients. PEM also performed as well as dedicated PET/CT in a comparison of images.
However, while there is a high correlation between PEM and radiography in these patients, the results are "not identical," the researchers noted. "The role of PEM in metabolic assessment and evaluating treatment response in inflammatory small joint disease warrants further exploration."
Mhlanga presented the study at the Society of Nuclear Medicine and Molecular Imaging (SNMMI) annual meeting in June.
PEM's primary purpose
With extremity imaging, x-rays mostly show established joint damage and occasionally show soft-tissue swelling and acute inflammation in patients with hand arthritis. Whole-body FDG-PET/CT can detect hypermetabolism in areas of inflammatory arthritis.
While PEM was designed for breast imaging, providing functional imaging at high resolution, dedicated small-joint imaging with PEM is "potentially well-suited to imaging inflammation in small synovial joints," according to Mhlanga.
The purpose of her study was to evaluate the performance of FDG-PEM in quantifying hand osteoarthritis, and to correlate PEM imaging with clinical signs, x-rays, and dedicated PET/CT scans.
The prospective study enrolled 14 patients (seven men and seven women) older than 21 years of age. The researchers divided the subjects into two groups: Eight patients comprised the osteoarthritis group and six patients formed a healthy control group of subjects with no abnormal symptoms or signs of the affliction.
The eight patients in the osteoarthritis group were undergoing whole-body FDG-PET/CT for known or suspected cancer. They agreed to additional hand imaging and were able to lie in a prone position for an eight-minute dedicated hand FDG-PET/CT scan.
The imaging protocol included PEM and x-ray imaging of both hands after the dedicated FDG-PET/CT scan. PET imaging was performed in two bed positions (4.3 minutes per position).
PEM technology
PEM was performed with a commercially available scanner (PEM Flex Solo I, Naviscan) using a protocol in which patients sat in a chair with their elbow resting on a table. Their hand was placed palm down on a lower detector head, while the upper detector head was pressed on the back of the hand to compress it, but without causing discomfort.
The space between the two PEM detectors was 4.5 cm to 6 cm, depending on the patient's wrist diameter. PEM imaging lasted for 10 minutes for a full field-of-view scan.
The PET/CT, PEM, and x-ray exams were randomly reviewed for each hand. A total of 32 hand joints per patient were evaluated, bringing the total number of joints analyzed to 442. The researchers reviewed the images for osteoarthritis, joint space narrowing, and any degree of malalignment, erosion, subchondral sclerosis, and subchondral inflammation.
For the radiography arm of the study, standardized three-view hand x-rays were scored for the severity of osteoarthritis using a modified Osteoarthritis Research Society International (OARSI) scoring method. Total joint glycolytic scores were obtained for PET/CT, while the total maximum standardized uptake value (SUVmax) on PEM was calculated for each joint.
In comparing the modalities, Mhlanga said they found a "significant difference between the PEM visual joint score [mean, 20.8 ± 4.2], as well as the PET/CT qualitative joint score [22.8 ± 5.38], which were higher in the osteoarthritic group compared to the control group."
The x-ray joint score (30.9 ± 31.3) was also significantly higher in the osteoarthritic group compared to the control group, as the researchers expected. The median score for the three modalities was 22.5.
 |
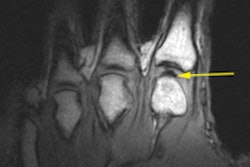
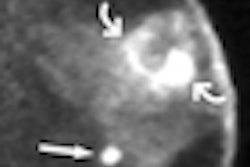
| Areas of uptake in the metacarpal joints show similarly on PEM (above) and PET/CT (below). There is evidence of joint space narrowing likely due to FDG uptake in areas of corrosive inflammatory osteoarthritis. All images courtesy of Dr. Joyce Mhlanga. |
 |
"There was significant correlation between the total quantitative PEM scores and the total FDG-PET/CT SUVmax score, as well as a significant correlation between the PEM visual score and PET/CT visual score," she added. "For some reason, we did not see a significant correlation between the quantitative scores of both PEM and PET, which may be due to the very small numbers of our [study] population."
A dedicated small-part PET system such as PEM "can provide high spatial resolution and joint imaging," Mhlanga and colleagues concluded. "High-resolution FDG-PEM imaging is feasible and performs at least as well as dedicated PET/CT."