ST. LOUIS - German researchers have developed a new PET radiotracer that detects recurrent prostate cancer in patients with very low prostate-specific antigen (PSA) levels, according to two preliminary studies presented on Sunday at the Society of Nuclear Medicine and Molecular Imaging (SNMMI) annual meeting.
Both studies evaluated the use of a gallium-68-labeled prostate-specific membrane antigen (PSMA) ligand with PET and were presented by lead author Dr. Matthias Eiber from Technische Universität München. The PET tracer was developed at the University of Heidelberg/Deutsches Krebsforschungszentrum (DKFZ) and used there primarily before coming to Technische Universität München.
In one study, 168 patients with a mean age of 61.8 years (range, 45-83 years) were imaged after receiving an injection of 128 MBq (± 16 MBq) of gallium-68 (Ga-68) PSMA. Contrast-enhanced PET/CT was performed on 116 patients, while 52 participants received PET/MRI, including multiparametric prostate MRI.
The median PSA level among the subjects was 1.8 ng/mL (range, 0.2-45 ng/mL). Prostate biopsies are often recommended when PSA levels rise above 4 ng/mL.
One nuclear medicine physician and one radiologist reviewed images in consensus, rating the results as suspicious or highly suggestive for recurrent prostate cancer, according to Eiber and colleagues.
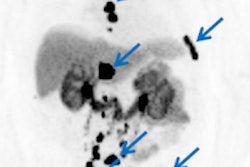
Of the 168 patients, 146 (87%) showed pathological uptake of Ga-68 PSMA. In those with a PSA level of 2 ng/mL or more, PET/CT's detection rate was 97% (64 of 66 patients), while PET/MRI had a detection rate of 93% (14 of 15 patients).
When PSA was 1 ng/mL to 2 ng/mL, PET/CT's detection rate was 93% (27 of 29 patients), compared with 90% (nine of 10 patients) for PET/MRI. When PSA was less than 1 ng/mL, PET/CT's detection rate was 67% (14 of 21 patients), compared with 59% (16 of 27 patients) for PET/MRI.
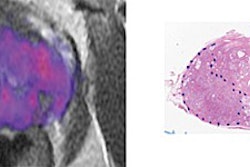
Eiber and colleagues also found that in patients with PSA less than 1 ng/mL, the combination of PET and multiparametric MRI increased definitive lesion localization in 48% of the subjects, compared with 29% for PET/CT.
Ga-68-PSMA-PET achieved a greater rate of detection for patients with recurrent prostate cancer than what has been previously reported for other tracers, especially at low PSA values, the researchers concluded. PET/MRI should be used in patients with PSA levels less than 1 ng/mL, as multiparametric MRI provides additional diagnostic information, they added.
Lymph-node staging
In the second study, Eiber and colleagues evaluated Ga-68 PSMA for use in preoperative lymph-node staging.
Ga-68-PSMA-PET imaging was performed on 37 intermediate- and high-risk prostate cancer patients. After injection of 131 MBq (±19 MBq) of Ga-68 PSMA, five patients underwent contrast-enhanced PET/CT and 32 received PET/MRI. All patients had a radical prostatectomy and extended pelvic lymph-node dissection.
The group used a five-point scale to assess all lymph-node stations. Depending on the uptake of Ga-68 PSMA in the primary tumor, patients were placed into group A (moderate to high uptake) or group B (no or faint uptake).
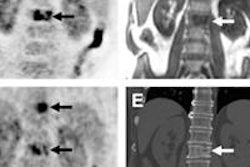
Histopathology revealed lymph-node metastases in 10 (27%) of the 37 patients and 19 (9%) of 214 stations. With Ga-68-PSMA-PET imaging, the primary tumor showed moderate to intense uptake in 33 (89%) of the 37 patients, while the other four patients (11%) had no uptake or faint uptake.
Patient-based analysis for group A showed a sensitivity of 75% and specificity of 96% for Ga-68 PSMA. With a field-based analysis, sensitivity was 65% and specificity was 98%. In group B, two patients showed lymph-node metastases that were not detected by PET.
"Our preliminary data show a moderate to high sensitivity for detecting lymph-node metastases in patients with PET-positive primary tumors," the researchers concluded. "However, our results also indicate that care must be taken in Ga-68-PSMA-negative primary tumors as lymph-node metastases appear to be PET-negative."