A percentage of children suspected of ingesting a foreign object may be able to avoid conventional bronchoscopy if virtual bronchoscopy is first performed, according to a study published in Emergency Radiology by Turkish researchers.
Researchers from Sisli Etfal Education and Research Hospital in Istanbul examined 45 children suspected of having tracheobronchial foreign body aspiration. They found that five of the children could have avoided an invasive procedure if radiologists had relied on the findings of virtual bronchoscopy images created from low-dose MDCT scans.
While conventional bronchoscopy remains the gold standard for diagnosing and managing foreign body aspiration, the researchers suggested that conventional bronchoscopies should not be performed unless either a chest radiograph or virtual bronchoscopy identifies a foreign body in the patient. Their findings were published online on November 19, 2008, in Emergency Radiology.
Between January 2005 and May 2007, 25 boys and 17 girls ranging in age from four months to 10 years who had received inconclusive chest x-rays were given virtual bronchoscopies with noncontrast CT from the larynx to the dome of the diaphragm (Somatom Sensation 16, Siemens Healthcare, Erlangen, Germany). Patients also received conventional bronchoscopy under general anesthesia.
Radiologists detected obstructive lesions in 35 of the 42 children from CT images and a virtual bronchoscopy fly-through. Thirty-four patients were diagnosed with foreign body aspiration and one with external compression, which was also confirmed by conventional bronchoscopy. Three mucoid plugs and two intrabronchial soft-tissue masses were misidentified as foreign body aspiration by radiologists when interpreting the virtual bronchoscopies. One foreign body was not identified in any of the MDCT scan images.
The radiation dose used for the CT scan was determined by the physical size of the patient (80 kVp, range of 20-80 mAs), according to radiologist Dr. Huseyin Ozkurt, the study's lead author. Images were of acceptable diagnostic quality at these low doses. CT scanning time ranged from five to eight seconds using a single breath-hold technique for patients who could comply and spontaneous scanning for children who could not.
Images with a slice thickness of 5 mm were recreated as axial, sagittal, and coronal images with a 0.75-mm slice thickness and 0.2-mm reconstruction interval on a dedicated advanced visualization workstation (Leonardo, Siemens Healthcare). Two radiologists initially interpreted these images, followed by a second interpretation after the images were reformatted as virtual bronchoscopies.
Conventional bronchoscopy confirmed 30 cases of tracheobronchial foreign body aspiration, including one case not identified by images from the CT exam or the virtual bronchoscopy. The overall sensitivity for virtual bronchoscopy was 96%, specificity was 58%, and positive/negative predictive values were 85% and 87%, respectively.
 |
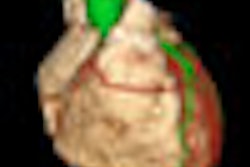
| Patient was a 24-month-old-boy hospitalized with sudden onset cough and dyspnea. Consecutive coronal VRT image shows a stenosis in the division of right intermediate and upper lobe bronchus. Also, the right lung shows hyperaeration due to air trapping (images at left and center). Virtual bronchoscopy image reveals obstruction in the right main bronchus (right). At bronchoscopy a piece of nut was removed. |
Ozkurt advocates that while chest x-ray should be the initial primary diagnostic imaging procedure to be performed, most aspirated foreign bodies could not be seen because food fragments have the same opacity as surrounding tissue. In this study, food fragments had been ingested by 90% of the patients who were diagnosed with a foreign body obstruction.
In addition to being noninvasive and not requiring sedation, an MDCT scan can reveal both a foreign body in the tracheobronchial tree and secondary pulmonary changes that can be useful in making a diagnosis. While virtual bronchoscopy is useful in evaluating the tortuous structure, detecting anatomic variations, and visualizing the bronchial system distal to obstruction, its most important disadvantage is that the foreign body may not be differentiated from other obstructive pathologies, the researchers noted.
By Cynthia E. Keen
AuntMinnie.com staff writer
January 30, 2009
Related Reading
3D penetrates trauma imaging niche, August 24, 2006
Copyright © 2009 AuntMinnie.com