Endocrinol Metab Clin North Am 2001 Jun;30(2):469-92
Isotope imaging for metastatic thyroid cancer.
Haugen BR, Lin EC.
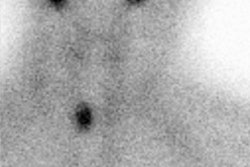
Many isotopes are available for imaging patients with suspected thyroid cancer
recurrence and metastases. TSH-stimulated low-dose 131I whole-body scanning with
serum thyroglobulin either by standard LT4 withdrawal or rhTSH stimulation is
the preferred test for monitoring patients without palpable disease or elevated
serum thyroglobulin on LT4 therapy (Fig. 5). This approach has the advantage of
finding disease that may be amenable to 131I therapy, although low-dose 131I
scans are less sensitive than are scans with other imaging agents. 123I has
better imaging characteristics than 131I and has been shown to be equivalent or
superior to low-dose 131I in recent studies. As the availability of 123I
increases and the cost decreases, this agent may replace 131I in imaging for
recurrent or metastatic thyroid cancer. Patients who have an elevated serum
thyroglobulin on LT4 therapy or after TSH stimulation but have a negative
low-dose 131I scan require other imaging procedures to find the suspected
disease. The authors currently perform a sensitive neck ultrasound to look for
surgically remediable disease and consider a noncontrast CT scan of the chest to
look for small pulmonary metastases that poorly concentrate low doses of 131I
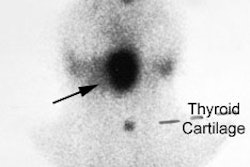
(Fig. 5). Fluoro-18-deoxyglucose PET, 99mTc MIBI, 201Tl, and 99mTc tetrofosmin
are primarily useful in the setting of a negative whole-body 131I scan and
elevated serum thyroglobulin. 18FDG-PET seems to have the highest sensitivity in
this setting and would be the preferred imaging agent, but availability and cost
are major issues (Fig. 5). Although some researchers have advocated these
radiopharmaceuticals as first-line agents replacing 131I, there is little
support for this position. This approach to imaging is not cost-effective
because positive scans in these patients would most likely require 131I
scintigraphy to determine whether the lesions are amenable to radioiodine
therapy. 99mTc pertechnetate, 99mTc furifosmin, and somatostatin receptor
scintigraphy have a limited role in imaging for recurrent or metastatic
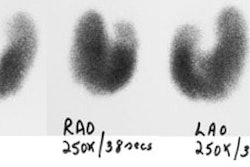
differentiated thyroid carcinoma. In choosing among 99mTc MIBI, 201Tl, and 99mTc
tetrofosmin, the technetium label of sestamibi and tetrofosmin results in better
image quality and faster imaging than 201Tl. Although 99mTc sestamibi and 99mTc
tetrofosmin have not been compared in a large series, the higher
tumor-to-background ratio and consistently high sensitivities of 99mTc
tetrofosmin suggest that it could potentially have additional value over 99mTc
sestamibi, but there is still limited experience with 99mTc tetrofosmin.