Metabolic Bone Disease:
Hyperparathyroidism:
Primary Hyperparathyroidism: It is important to remember that between 50 to 80% of patients with primary hyperparathyroidism will have a normal bone scan. In general, only advanced cases of the disorder demonstrate findings on the bone scan. Increased activity on delayed images can be seen in the axial skeleton, the long bones, the mandible, the skull, the acromioclavicular joints, hands, and the sternum (areas which frequently demonstrate demineralization on plain film). Focal abnormalities can be seen in association with Brown tumors, or compression fractures. Soft tissue accumulation of the tracer can be seen in sites of metastatic calcification (particularly the lungs, kidneys, and stomach).
Secondary Hyperparathyroidism: Unlike primary hyperparathyroidism, the bone scan in patients with secondary hyperparathyroidism is usually abnormal. There is diffusely increased skeletal activity, with decreased renal activity producing a "super scan" appearance. Beading of activity may be seen along the costochondral junctions. Brown tumors may also produce focal abnormalities.
Osteomalacia:
Osteomalacia is characterized by a normal volume of bone with diminished mineralization of the organic matrix. It is associated with vitamin D deficiency. It may occur due to acquired disorders of vitamin D metabolism, gastrointestinal or hepatic disease, or in association with secondary hyperparathyroidism due to end-stage renal disease. Patients generally complain of bone pain, with striking tenderness. On plain films, the bones are osteopenic. Pseudofractures (Looser zones) appear as bands of deossification, 2 to 3 mm wide, located at one side of a bone or extending across its entire width. Common sites include the outer border of the scapula, femoral neck, pubic rami, proximal ulna, distal radius, ribs, and clavicles. Pseudofractures are typically symmetric.
On delayed bone scan osteomalacia frequently demonstrates diffusely increased skeletal uptake which can be indistinguishable from other metabolic bone disorders. Pseudofractures appear as focal areas of increased tracer activity in the previously described common locations.
Hyperthyroidism:
In hyperthyroidism, rates of both bone resorption and bone formation are increased. Despite the fact that resorption tends to predominate, demineralization is generally not observed on radiographs. The bone scan in these patients may demonstrate diffusely increased osseous activity (Super scan appearance).
Pagets Disease:
Pagets disease affects between 3% to 4% of the population over the age of 40 years and up to 10-11% after age 80 years [1]. Although the actual cause of Pagets disease is not known, a viral etiology has been postulated due to the presence of intra-nuclear inclusion bodies which resemble viral nucleocapsids within the osteoclasts of Pagetoid bones [1]. The most commonly involved bones are the vertebral bodies (30-75%), skull (25-65%), pelvis (30-75%), and proximal long bones (25-30%) [1]. Monostotic disease occurs in 10-35% of cases and is more often seen in the axial skeleton [1]. Polyostotic disease (65-90%) occurs more commonly [1]. Symptoms include pain, bowing deformities, kyphosis of the spine, and bone enlargement [1]. About 20% of affected patients are initially asymptomatic [1].
There are generally considered to be 3 phases to the disorder- lytic phase, mixed phase, and blastic phase. Initially, intense osteoclastic activity produces the lytic or incipient active phase. Lytic findings are more commonly seen in the skull and long bones. In the skull, involvement is refered to as osteoporosis circumscripta which produces well defined areas of lucency in the occipital and frontal bones [1]. The is notable absence of peripheral sclerosis surrounding the lucent areas [1]. Both the inner and outer calvarial tables are involved [1]. In the long bones, the process begins in the subchondral area of the epiphysis and extends along the shaft in a characteristic wedge-shaped ("flame" or "blade of grass") appearance. The lytic phase is followed by the mixed or fibrous phase in which bone marrow is replaced by very vascular fibrous tissue. There is coarsened thickening of the trabecular pattern and cortex [1]. In the vertebral bodies, osteoblastic activity is seen along all 4 margins producing a "picture frame" appearance [1]. There is also "squaring" of the normal concavity of the anterior margin of the vertebral body [1]. Disorganized ossification and deformities or fractures may occur. Finally, the disorder become quiescent with the involved bone generally appearing enlarged and sclerotic.
During the lytic portion of the disease lesions may demonstrate uniform increased tracer accumulation, or may have relative photopenia in their center producing a "donut" appearance. In the long bones, increased tracer activity is particularly prominent along the advancing edge of the disorder. Scintigraphy is more sensitive than plain films for disease detection and extent during the lytic phase.
During the fibrous phase, the bone scan demonstrates marked
increased uptake of tracer
in the involved areas. The bone scan can be used to document the
effectiveness of therapy
in these patients. Later, during the sclerotic phase, the bone
scans will begin to show
less intense tracer accumulation and may become normal.
At FDG PET, bones involved by Paget disease most commonly exhibit
no abnormal uptake [2]. Less commonly, marked cortical FDG uptake
with sparing of the medullary cavity may be seen [2].
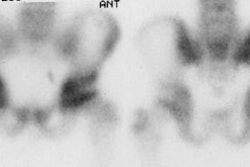
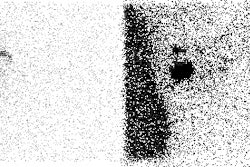
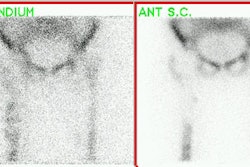
|
Pagets Disease: Multiple sites of involvement by Pagets disease including the jaw. |
|
|

Sarcomatous degeneration occurs only rarely in Pagetoid bone (about 1% of patients [1]). Patients with severe polyostotic disease have an increased risk for degeneration (up to 5-10%) [1]. Males are affected more than females (2:1) [1]. New focal pain and swelling are the most common clinical complaints [1]. The most common location is the hip, pelvis, and shoulder [1]. The most common neoplasm is an osteosarcoma (50-60% of cases [1]), but chondrosarcoma, fibrosarcoma, and malignant fibrous histiocytomas have all been described. Radiographs may show a new, enlarging lytic lesion. Bone scan commonly reveals decreased uptake of tracer within the lesion in comparison to the adjacent Pagetoid bone, however, increased activity may also be seen.. The loss of tracer uptake may be because many of these malignant lesions are lytic on plain film, or the finding may be secondary to necrosis within the tumor. Increased gallium accumulation associated with relatively decreased Tc-MDP activity suggests malignant degeneration.
REFERENCES:
(1) Radiographics 2002; Smith SE, et al. Radiologic spectrum of Paget disease of bone and its complications with pathologic correlation. 22: 1191-1216
(2) Radiographics 2016; White ML, et al. Specturm of benign
articular and periarticular findings at FDG PET/CT. 36: 824-839