A committee of lung experts from various respiratory societies has prepared a new guideline for diagnosing idiopathic pulmonary fibrosis (IPF) using high-resolution CT scans. The guideline is available in the September issue of the American Journal of Respiratory and Critical Care Medicine.
The 2018 clinical practice guideline for IPF aims to refine the criteria used to identify the rare and often fatal lung disease based on new evidence accumulated since the previous guideline was published in 2011.
IPF is challenging to diagnose because its symptoms are nonspecific and common to most interstitial lung diseases, Dr. Ganesh Raghu from the University of Washington noted in a release from the university. Raghu served as chair of the 29-member guideline committee, which included representatives from the American Thoracic Society, the European Respiratory Society, the Japanese Respiratory Society, and the Latin American Thoracic Society.
In preparing the new guideline, the committee accumulated evidence from all relevant studies and rated the strength of their findings using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) protocol (Am J Respir Crit Care Med, September 2018, Vol. 198:5, pp. e44-e68).
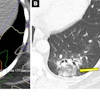
Their review led to the development of four distinct categories when diagnosing IPF using data from high-resolution CT scans: usual interstitial pneumonia (UIP) pattern, probable UIP pattern, indeterminate pattern, and alternative diagnosis.
The committee also offered several suggestions to clinicians evaluating adult patients suspected of having IPF, including the following:
- Take a detailed history of a patient's medications and environmental exposures, and perform serological testing to rule out connective tissue disease.
- Use bronchoalveolar lavage or surgical lung biopsy for patients with probable UIP pattern, indeterminate pattern, or alternative diagnosis, but not for those with a UIP pattern.
- Hold a multidisciplinary discussion between pulmonologists, radiologists, and pathologists before diagnosing IPF.
- Do not measure blood biomarkers just to distinguish IPF from other interstitial lung diseases.