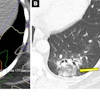
Although two commercially available AI software applications can yield different volume estimations on stroke CT perfusion (CTP) studies, the differences aren't significant enough to affect patient eligibility for thrombectomy, researchers reported in an article published May 2 in the Journal of Stroke Cerebrovascular Diseases. However, there are still important issues to be aware of.
In a study involving 362 stroke cases, researchers led by first author Benjamin Alwood, MD, in the department of vascular neurology at the University of Florida in Jacksonville, and colleagues, compared core and penumbra volumes estimated by AI stroke detection software from Viz.ai and Rapid AI and assessed DEFUSE-3 thrombectomy eligibility. While there were systematic differences in estimates between the software applications, DEFUSE-3 thrombectomy eligibility wasn't statistically different. However, they did find one eligibility difference on one scanner at one institution, suggesting that scanner model and local CTP protocols can influence performance and cause discrepancies in thrombectomy eligibility.
"We thus recommend centers discuss optimal scanning protocols with software vendors and scanner manufacturers to maximize CTP accuracy," the authors wrote.
Studies were performed on 10 scanners from four different manufacturers: four Aquilion One (Canon Medical Systems), three Discovery scanners (GE HealthCare), one Revolution scanner (GE), one Ingenuity scanner (Philips), and one Somatom Definition Flash scanner (Siemens Healthineers). Each scanner utilizes a slightly different scanning technique to optimize performance and radiation dose, resulting in slightly different image quality and temporal resolution, the authors noted. Alwood and team analyzed CTP data of acute stroke patients with large vessel occlusion (LVO) from four institutions.
- At Center A, Rapid.AI was used from 2018-2021 to process CTP images on patients with CTA-diagnosed LVO in the 6-24 hour window. The original imaging data was retrospectively reprocessed with Viz.ai for the purposes of this study. The remaining three centers used Viz.ai and Rapid.AI simultaneously to process CTP volumes.
- Center B routinely scans all stroke codes with CTP; data from Jan 2021 to July 2022 were screened.
- Center C used CTP in acute stroke patients with NIHSS ≥ 4 or for CTA-confirmed LVO; data from Dec 2022 to March 2023 were screened.
- Center D used CTP in acute stroke patients with NIHSS ≥ 5 or for CTA-confirmed LVO; data from Jan 2022 to March 2022 were screened.
Results between the software packages were compared and categorized by National Institutes of Health Stroke Scale (NIHSS) score, scanner manufacturer/model, and institution.
Alwood et al found both Viz.ai software core volumes and Viz.ai penumbra volumes showed significantly higher measures than Rapid.AI. These differences were primarily driven by Canon Aquilion One scanners at two separate institutions, the authors said.
For example, Viz.ai's software provided larger estimates with mean differences of 8cc and 18cc for core and penumbra, respectively (p < 0.001). An NIHSS subgroup analysis also showed systematically larger Viz.ai volumes (p < 0.001).
"Despite volume differences, in this case, a significant difference in thrombectomy eligibility was not found," the authors wrote.
On the other hand, additional subgroup analysis showed significant differences in penumbra volume for the Philips Ingenuity scanner, and thrombectomy eligibility for the Canon Aquilion One scanner at one center (7% increased eligibility with Viz.ai, p = 0.03).
"Despite systematic differences in core and penumbra volume estimates between Viz.ai and RAPID.AI, DEFUSE-3 eligibility was not statistically different in primary or NIHSS subgroup analysis," Alwood and team concluded. "A DEFUSE-3 eligibility difference, however, was seen on one scanner at one institution."
The researchers noted that their results highlight the inherent challenges and uncertainties of using CTP for determining thrombectomy eligibility.
Read the full report here.