Emergency department physicians improved their ability to predict acute coronary syndrome (ACS) by adding a T2-weighted sequence to their cardiac MRI protocol, according to a new study from Harvard Medical School and Massachusetts General Hospital in Boston. The results, reported in Circulation, suggest that MR might do a better job of triaging chest pain patients compared to standard risk assessments.
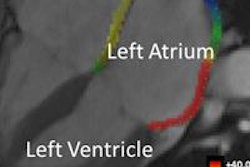
Adding the T2-weighted MR sequence enabled doctors to visualize edema in the myocardium, a primary sign of acute injury, the researchers explained. Armed with the ability to distinguish new from old myocardial infarction, they could better predict which patients were at high risk for ACS and which could safely be sent home.
Many patients presenting to the emergency department with chest pain are at risk of ACS, even though initial biomarkers of cardiac injury and electrocardiogram (ECG) changes may be nondiagnostic, wrote principal investigator Dr. Ricardo Cury, assistant professor of radiology at Harvard Medical School, along with Dr. Khalid Shash, Dr. John Nagurney, and colleagues.
The potentially catastrophic consequences of discharging patients at risk of ACS lead to many unnecessary hospital admissions.
"Approximately 30% of patients admitted for suspected myocardial infarction (MI) are eventually diagnosed with ACS," they wrote. "On the other hand, 2% to 4% of patients with chest pain discharged from hospital EDs experience an ACS within 30 days. A possible strategy to triage these patients includes the early use of cardiovascular imaging for rapid diagnosis and appropriate management" (Circulation online, August 4, 2008).
In 2004, Abdel-Aty and colleagues reported that T2-weighted cardiac magnetic resonance (CMR) imaging could be used to differentiate acute from chronic myocardial infarction (Circulation, May 25, 2004, Vol. 109:20, pp. 2,411-2,416). Cury and his team assessed the preliminary results of such a strategy in the emergency department, and they also evaluated whether MRI provided incremental value to the initial risk assessment in the emergency department based on standard risk factors.
"It is well known that patients with chronic MI have left ventricular [LV] wall thinning," Cury and his colleagues wrote. "Our hypothesis was that a comprehensive CMR protocol that used cine wall motion, rest first-pass myocardial perfusion (FP-MRI), T2W images, LV wall thickness (LVWT) analysis, and delayed-enhancement imaging (DE-MRI) could significantly increase the detection of ACS compared with existing triage strategies in patients presenting with chest pain in the ED."
To that end, the team enrolled a prospective cohort of patients presenting to the emergency department with acute chest pain and negative cardiac biomarkers and without ECG changes that would indicate the presence of acute ischemia.
All 62 patients in the cohort were awaiting admission to the hospital for a rule-out MI protocol. To eliminate those with a very low likelihood of MI, the study eliminated patients who were not being admitted. Elevated troponin levels, ECG changes, and contraindications to MRI were among the exclusion criteria. During their hospitalization, the patients received standard clinical care to rule out ACS, including exercise performance, stress perfusion imaging, or cardiac catheterization as indicated clinically, in addition to MRI.
The subjects were scanned on a 1.5-tesla scanner (Signa HDx, GE Healthcare, Chalfont St. Giles, U.K.) equipped with an eight-element phased-array cardiac coil. After injection of 0.1 mmol/kg of gadopentetate dimeglumine (Gd-DTPA, Bayer Schering Pharma, Berlin) at two points during the exam, patients were scanned in a protocol that included T2-weighted imaging, FP-MRI, cine left ventricular function in two- and four-chamber views, DE-MRI, and assessment of ventricular wall thickness.
After the first bolus injection, a black-blood T2-weighted double-inversion recovery sequence with a fat-saturation pulse was performed at two RR intervals; echo time 100 msec, echo train length 20; matrix 256 x 256; field-of-view 32 to 34 cm; slice thickness 12 mm, the authors noted. This was followed by breath-hold FP-MRI myocardial perfusion imaging, performed with a hybrid gradient-echo planar imaging pulse sequence during a second bolus injection, and a saline flush allowing the acquisition of five to eight slices in the short-axis view.
While the contrast was washing out of the myocardium, cine images were acquired with steady-state FP-MRI in the short-axis view. Approximately 10 minutes after the second contrast injection, DE-MRI images were acquired using a gated, fast gradient-echo pulse sequence by an adiabatic 3D technique, with 2D views added as necessary.
The primary end point of the study, clinical outcomes, was assessed by an expert panel using American Heart Association (AHA) and American College of Radiology (ACR) guidelines. The diagnostic accuracy of each CMR technique was evaluated separately.
Two experienced readers, blinded to all clinical data, evaluated the images in consensus. They looked for edema, myocardial perfusion defects, wall motion abnormalities, delayed hyperenhancement, and left ventricular wall myocardial thinning.
In all, 13 of 62 patients (21%; 95% confidence index [CI]) developed ACS during their index hospitalization period, Cury and his team reported. The new CMR protocol, which added a T2-weighted scan and assessment of ventricular wall thickness, yielded increases in the specificity, positive predictive value, and overall accuracy from 84% to 96%, 55% to 85%, and 84% to 93%, respectively, compared to the conventional CMR protocol. Sensitivity remained unchanged at 85%, with a slight increase in the negative predictive value.
Logistic regression analysis of the new CMR protocol that included information on clinical risk assessment (c-statistic = 0.695) and traditional cardiac risk factors (c-statistic = 0.771) showed an improvement in the c-statistic to 0.958 (p < 0.0001).
"We demonstrated that the addition of CMR in the evaluation of these patients is highly accurate for the detection of patients with ACS and provides incremental value to initial clinical risk assessment and traditional risk factors," Cury and colleagues wrote. The new protocol improved the overall accuracy of CMR with improvements in the specificity and positive predictive values.
"In the comparison between the individual MRI parameters, T2-weighted imaging allowed 100% specificity but 69% sensitivity. On the other hand, LVWT analysis allowed poor specificity (10%) but excellent sensitivity (100%)," they wrote. "One can assume from these data that if T2-weighted imaging is positive, the patient has ACS (positive predictive value 100%), and conversely, if LV thinning is present, the patient does not have ACS and has had a prior chronic MI."
Locating the MRI system directly in the emergency department was another advantage of the study, allowing the scans to be performed in a timely manner.
There are other useful exams for evaluating chest pain patients in the emergency department, including contrast echocardiography, SPECT myocardial perfusion imaging, and coronary CT angiography, the authors noted.
"Although these imaging modalities are useful in excluding ACS (because of their high negative predictive value), they are not entirely helpful in identifying patients with true ACS and thereby refining patient management in those who need more aggressive treatment, because they are limited by low to intermediate positive predictive values," they wrote. The ability of the new protocol to rapidly identify chest pain patients with unstable angina and non-ST-segment elevation MI (NSTEMI), as well as myocardial areas at risk, could lead to quick, targeted revascularization strategies, they added.
Limitations of the study included the small sample size, low availability of scanners capable of performing in emergency departments, and the inherently low signal-to-noise ratio of fast spin-echo T2-weighted imaging.
In this pilot study, CMR showed a high diagnostic accuracy for identifying patients with ACS and provided additional value over standard and institutional cardiac risk factors, Cury and his colleagues wrote.
"Future studies will need to confirm these observations in a larger trial, determine the impact of CMR in clinical decision-making, and assess the cost-effectiveness of CMR in the ED setting," they concluded.
By Eric BarnesAuntMinnie.com staff writer
August 15, 2008
Related Reading
Most U.K. patients don't undergo needed coronary angiography, April 25, 2008
Women with angina and normal coronary arteries fare worse than similar men, March 7, 2008
MR-IMPACT trial: CMR equivalent to SPECT for stenosis detection, February 18, 2008
Dipyridamole stress cardiovascular MRI predicts CAD outcomes, October 11, 2007
Cardiac MR measures predict pulmonary hypertension, April 9, 2007
Copyright © 2008 AuntMinnie.com