J Nucl Med 1994 Feb;35(2):257-62
Serum thyroglobulin and iodine-131 whole-body scan in the diagnosis and
assessment of treatment for metastatic differentiated thyroid carcinoma.
Lubin E, Mechlis-Frish S, Zatz S, Shimoni A, Segal K, Avraham A, Levy R,
Feinmesser R.
Because of the limitations of periodic 131I whole-body scans, including
suspension of substitution therapy, questionable sensitivity and low yield in
detecting metastases in patients who have undergone thyroidectomy, serum
thyroglobulin and 131I whole-body scans were evaluated for sensitivity in
detecting local, regional or distant metastases in 261 patients with
differentiated thyroid carcinoma after total thyroidectomy and ablation.
METHODS: A noncompetitive immunoradiometric assay was used for serum
thyroglobulin determination. An 131I whole-body scan was obtained after
replacement therapy had been suspended for 6 wk or when TSH reached levels
higher than 50 microU/ml. In patients who underwent radiological procedures with
iodinated contrast media, the waiting period before the 131I whole-body scan was
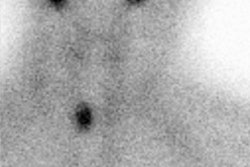
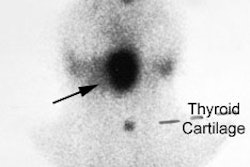
no less than 10 wk. RESULTS: Of the 58 patients with proven metastases who were
followed for 12 yr (mean 7 +/- 3.3 yr), 51 (88.4%) had high serum thyroglobulin
assays performed while under full replacement therapy and 32 (55%) showed clear
131I whole-body scan localization. There were no instances of positive
whole-body scans and negative serum thyroglobulin. CONCLUSION: In patients
treated with 131I, serum thyroglobulin assay was an excellent method to assess
treatment. Patients with metastatic disease and negative whole-body scans with
or without serum thyroglobulin exhibited a trend toward higher mortality. This
trend may also indicate that the lack of 131I trapping and low thyroglobulin is
a sign of metabolic dedifferentiation of otherwise histologically differentiated
thyroid tumors.