J Nucl Med 2001 Oct;42(10):1470-5
Serum thyroglobulin concentrations and (131)I whole-body scan results in
patients with differentiated thyroid carcinoma after administration of
recombinant human thyroid-stimulating hormone.
David A, Blotta A, Bondanelli M, Rossi R, Roti E, Braverman LE, Busutti L, degli
Uberti EC.
The use of recombinant human thyroid-stimulating hormone (rhTSH) has recently
become available as an alternative diagnostic tool to assess the persistence and
recurrence of differentiated thyroid carcinoma (DTC) in patients on thyroid
hormone-suppressive therapy (THST) after near-total or total thyroidectomy and
ablative doses of (131)I. We report the results of rhTSH administration in
patients who were monitored for DTC. METHODS: Thirty-three adult DTC patients
(13 men, 20 women; mean age +/- SE, 45.6 +/- 2.31 y; age range, 21-65 y)
underwent diagnostic follow-up after rhTSH administration at a dose of 0.9 mg
once a day for 2 d. Whole-body scanning and serum thyroglobulin (Tg) measurement
were performed after rhTSH administration. Patients were divided into 2 groups
depending on serum Tg concentrations on THST: 29 patients had Tg concentrations
of <2 ng/mL (group A) and 4 patients had Tg values of >2 ng/mL (group B).
RESULTS: In group A, Tg values remained at <2 ng/mL in 25 patients and
increased from 1.1 +/- 0.14 ng/mL to 22.0 +/- 5.75 ng/mL (mean +/- SE) in 4
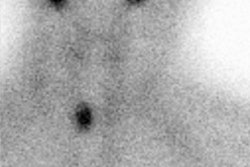
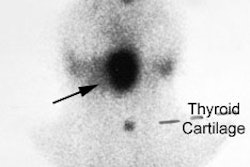
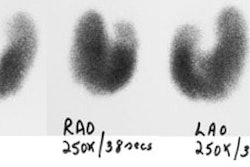
patients after rhTSH administration. Whole-body scanning did not reveal any
uptake of (131)I in the 25 patients without an increase in Tg, whereas (131)I
uptake was evident in 2 of the 4 patients with a rise in Tg. In group B, Tg
values increased in all 4 patients from 17.3 +/- 6.35 ng/mL to 55.3 +/- 12.75 ng/mL,
and (131)I uptake was evident in 3 of the 4 patients. No major adverse effects
were reported after rhTSH administration. CONCLUSION: Our results show that the
measurement of serum Tg concentrations after rhTSH has a higher diagnostic value
than whole-body scanning in detecting the persistence of thyroid tissue.
Therefore, rhTSH should be administered in TSH-suppressed patients with basal
serum Tg concentrations of <2 ng/mL because the increment in serum Tg
concentrations may reveal the persistence of thyroid tissue in these patients.