Distinguishing juvenile idiopathic arthritis (JIA) from other diseases is critical because management of the various conditions can differ substantially. Now a British group is highlighting the distinctions between JIA and a rare genetic disorder known as camptodactyly-arthropathy-coxa vara-pericarditis (CACP) syndrome.
The syndrome can mimic both polyarthritic and systemic JIA according to the authors, led by radiologist Dr. Amaka Offiah of London's Great Ormond Street Hospital for Children. The group's pictorial essay is published in the latest issue of the American Journal of Roentgenology (AJR, August 2005, Vol. 185:2, pp. 522-529).
But while children with CACP syndrome often have joint effusion, CACP syndrome is not an inflammatory disorder and doesn't respond to the steroids or other anti-inflammatory drugs used for JIA.
The authors state that CACP syndrome is probably underdiagnosed. The syndrome is currently managed with intensive physiotherapy, as no medication has been shown to improve the arthropathy.
As might be expected, camptodactyly is a characteristic feature of CACP syndrome but one that isn't always obvious on x-rays, according to the authors. Coxa vara with short femoral necks can also been seen in radiographs of the pelvis.
 |
| Fourteen-year-old boy with camptodactyly-arthropathy-coxa vara-pericarditis (CACP) syndrome. Anteroposterior radiograph of pelvis shows smooth flattening of femoral heads and acetabulae are irregular. Initial cursory examination may suggest erosive change; however, presence of large acetabular cysts, particularly on the left (arrows) is virtually pathognomonic of CACP syndrome and is highly unusual in juvenile idiopathic arthritis. Note also bilateral coxa vara, which is a feature of condition. |
Periarticular osteopenia may appear on radiographs of CACP syndrome patients, but it is less pronounced than that seen with JIA. The syndrome also causes nonerosive arthropathy with smooth flattening of the affected joint surfaces, the authors stated.
Some highly distinguishing features of CACP syndrome are intraosseous fluid-filled herniations affecting the acetabulum that appear on x-rays as benign radiolucent acetabular lesions.
"The characteristically large acetabular cysts that occur in CACP syndrome are not seen in juvenile idiopathic arthritis," the authors noted. Also unlike JIA, the cervical spine in CACP syndrome remains normal.
Another characteristic aspect of CACP syndrome is visible in the hands, in the squaring of the metacarpal and phalangeal heads.
 |
| Fourteen-year-old boy with camptodactyly-arthropathy-coxa vara-pericarditis (CACP) syndrome. Dorsopalmar radiograph of left hand illustrates that presence of camptodactyly may not always be obvious from radiographs. Arthropathy in CACP syndrome may be associated with periarticular osteopenia. Note absence of erosive change. Although this appearance is consistent with early juvenile idiopathic arthritis, squaring of metacarpals and phalanges (seen in CACP syndrome) helps to differentiate two conditions. Amaka OC, Woo P, Prieur A, Hasson N, Hall CM, "Camptodactyly-Arthropathy-Coxa Vara-Pericarditis Syndrome Versus Juvenile Idiopathic Arthropathy" (AJR 2005; 185:522-529). |
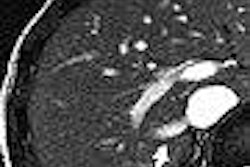
"MRI of patients with CACP syndrome clearly depicts large joint effusions, confirms the fluid nature of the radiolucent acetabular herniations seen on radiography, and shows their intra-articular connection," the authors wrote.
"Enhancement of the mildly thickened synovial lining of the joint capsule and absence of cartilage destruction are said to be characteristic," the authors continued. "However, in more advanced or long-standing disease, loss of joint space, signifying cartilage destruction, may occur without erosive change."
In summation, the AJR authors make a pitch for increased awareness of CACP syndrome to avoid confusing it with other childhood musculoskeletal conditions, especially JIA.
"Differentiation from juvenile idiopathic arthritis is clinically important in view of the different management of the two conditions and in particular because of the possible severe side effects of juvenile idiopathic arthritis treatment," they concluded.
By Tracie L. Thompson
AuntMinnie.com staff writer
August 10, 2005
Related Reading
Pinhole SPECT shows promise for arthritis imaging, July 22, 2005
MRI, x-ray yield comparable sensitivities for RA joint erosion, June 10, 2005
Juvenile idiopathic arthritis linked to reduced bone mass gains, March 21, 2005
MRI and CT: Complementary techniques in assessing rheumatoid arthritis, March 9, 2005
Power Doppler shows promise in juvenile RA, January 7, 2005
Copyright © 2005 AuntMinnie.com