Few things can dampen the results (and the spirits) of chest radiologists like a CAD application that finds too many false-positive lung nodules. Even experienced radiologists who work with CAD every day can find the false positives vexing.
And the situation could be worse than they think. A recent preliminary study found that radiologists tended to accept CAD's bad choices when the former spent too much time at the CAD workstation. But that's another story.
At the recent Computer Assisted Radiology and Surgery (CARS) conference in Osaka, a researcher from Canada presented a CAD algorithm that can distinguish between faint and similarly shaped lung structures, reducing false positives with the aid of a hybrid learning scheme that uses both linear discriminant analysis and fuzzy c-means clustering. To achieve these results the group integrated two methods that have shown promising results individually.
The results, tested so far only on a small pediatric dataset, nevertheless represent a significant improvement over other recent studies, according to Javad Alirezaie, Ph.D., who presented the data. Alirezaie is from the engineering department of Ryerson University in Toronto and the University of Waterloo in Waterloo, Ontario.
"The proposed scheme is hybrid in the sense that it combines the discrimination power of fuzzy c-means clustering with the classification ability of a modified version of LDA (linear discriminant analysis) to achieve false-positive reduction," wrote Alirezaie and colleagues Negar Memarian and Dr. Paul Babyn, radiologist in chief at the Hospital for Sick Children in Toronto and an associate professor at the University of Toronto, in their abstract.
"The first module of this scheme provides an estimate of the number of nodules for each patient through fuzzy c-means clustering (unsupervised learning)," they wrote. "The second step is what we have designed and named adaptive iterative LDA (supervised learning). This step is used for futher redction of FPs (false positives) when the fuzzy c-means clustering has determined the existence of multiple nodules."
The method was developed for and tested on a pediatric population, typically children with lung metastases rather than primary malignancies, Alirezaie explained. There are differences between these nodules and those of adult smokers who make up the typical CT lung screening cohort, for example. But the method matters more than the cohort, according to Alirezaie, who suggested that pediatric metastases might be harder to detect.
The proposed scheme, which involved integrating two tested methods for reducing false positives, could potentially "enhance the performance of any lumen-based lung CAD system," he said. The goal was to detect all types of nodules, including central, peripheral, pleural, and those adjacent to blood vessels.
"The first step is ROI (region of interest) detection, which is extraction of the lung data," Alirezaie said. "The next step is detection of potential nodule candidate in lungs, and (step) three, removing false-positive detections."
For each nodule candidate, nine features are selected and extracted including "mean intensity of the nodule; mean intensity of the nodule surrounding; morphologically the access ratio, compactness, area, and volume; and contexual area -- the perimeter, the vertical ratio, and the position of the nodule in the lung context," he said. "That means for every nodule candidate in the first step we do the ROI and we find all these nine features."
 |
| Nodules detected by ROI detection system. Top, small nodule with inconspicuous intensity difference with surrounding lung context. Below, small well-formed nodule. Third from top, small nodule hardly distinguishable from the background and nearby thin vessels. Bottom, small irregularly shaped nodule. All images courtesy of Javad Alirezaie, Ph.D. |
 |
 |
 |
Next, in fuzzy c-means clustering, the findings are deemed nodules or non-nodules based on their area and compactness. Based on these two features, which proved to be the most effective for cluster determination, each sample is assigned a "membership grade" of 0 or 1, indicating no membership or full membership, respectively, Alirezaie said. Grades between 0 and 1 are given partial membership in a cluster.
Fuzzy c-means clustering then optimizes the location of the clusters, with the algorithm updating itself by minimizing a cost function at each iteration. Once the results of this process converge, a thresholding step is applied: for each CT dataset, if the number of objects clustered is smaller than the threshold, the results are considered false-positive and excluded from further analysis. The threshold is equal to 5% of the total number of candidates in the case with the lowest number of detected objects, according to the abstract.
CT datasets that have multiple members in the nodule cluster are then processed with linear discriminant analysis for more cautious classification. The LDA analysis is adaptive in that it seeks the appropriate level of discrimination for each CT image. It is cautious in that it assigns a prior probability of 95% for membership in a nodule group (5% for membership in a non-nodule group) to preserve as many true positives as possible, the researchers wrote.
"If the total number of candidates in a nodule group at one iteration is different from that of the iteration before it" and less than a cutoff threshold, the current LDA threshold is determined to have been unable to find many false positives, and so the membership probabilities are altered by 5% at each successive pass, the group explained.
Unlike previous schemes that used fixed thresholds for discriminant analysis of nodule candidates, "the present approach updates its discrimination level based on the information attained from previous iterations of LDA," they wrote.
The process was tested on 24 pediatric patients from the Hospital for Sick Children in Toronto (which is affiliated with the University of Toronto), who were imaged with CT using 5-mm slices, Alirezaie said. The first 19 patients included in the abstract yielded 947 CT images and 239 metastatic true nodules, 41 of which were smaller than 4 mm and 28 of which were smaller than 3 mm.
"The results we have obtained after the morphological operation (yielded) sensitivity from 76% to 77%" and a high false-positive rate, Alirezaie said. "After the second step, which is shape featuring, we reduced the false positives to 2.79.... By introducing the enhanced false-positive reduction scheme, we were able to reduces FPs to 2.4 for different sets of data."
The results showed "good improvement over the original results generated by the automatic rule-based lung nodule detection system, which had 80% sensitivity and 3.05 FPs per slice," the team wrote. "This means that the false-positive rate is nearly halved (from the group's previous CAD system) ... while a good level of sensitivity is retained. The lowest FP per slice is achieved when all nine features are used in the iterative LDA. The next most discriminant set of features are the contextual features (78.24%, 1.67 FP per slice) emphasizing the fact that position of the nodule candidate wtihin lung context is important."
By way of comparison, a 2005 study in adults yielded a 70% sensitivity with 1.67 FP detections per slice, Alirezaie noted (Academic Radiology, March 2005, Vol. 12:3, pp. 337-46).
 |
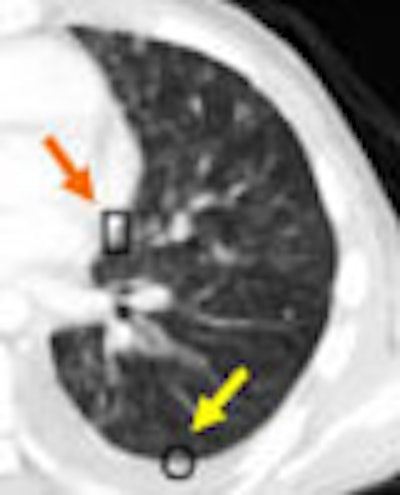
| An example of successful nodule classification. The circle encloses a true wall nodule. The rectangle surrounds a very similar wall object that is in fact a false positive erroneously detected by the group's previous CAD system. The current hybrid FP reduction approach recognizes and removes this false-positive finding. |
The present study may be the first in Canada to focus on lung CAD in the pediatric population, he said, noting that use of a pediatric cohort rather than adults may have affected the results.
 |
| An example of successful nodule classification. Above, bright well-formed true nodules marked inside circles. Below, very similar non-nodule objects marked inside rectangles. The hybrid FP reduction stage accurately categorizes these objects as false positives. |
 |
In any case, "we have developed a scheme to detect ... a broad range of interior and juxtapleural nodules as small as 2.23 mm," Alirezaie said. Yielding 72% sensitivity at 2.4 false positives per patient at its final step, the method reduced false positives by 38% over the group's earlier CAD system, and "should raise the performance in presenting nodules that are hardly distinguishable from non-nodular components."
The method could potentially be used as an enhancing step for other lung CAD schemes, Alirezaie said. Future plans include expanding the patient cohort and "adding more features for training and testing the classifier."
By Eric Barnes
AuntMinnie.com staff writer
July 24, 2006
Related Reading
Lung CAD may lead radiologists down the wrong path, June 16, 2006
CAD improves lung nodule detection, June 1, 2006
Part II: Automated CT lung nodule assessment advances, May 16, 2006
Part I: Automated CT lung nodule assessment advances, April 17, 2006
Trimming CT dose decreases lung CAD performance, January 12, 2006
Management strategies evolve as CT finds more lung nodules, August 19, 2005
Copyright © 2006 AuntMinnie.com