CT appears to have a useful way of demonstrating the noncalcified lipid-rich plaques that are at risk of rupturing -- at least the larger ones, according to researchers from Massachusetts General Hospital (MGH) in Boston.
The MGH team found that CT depiction of the so-called napkin-ring sign (NRS) was independently linked to the size of the necrotic or lipid plaque core and the noncore plaque, as well as the vessel area based on histology. As a result, CT and invasive intravascular ultrasound may share an ability to find vulnerable coronary artery plaques before they are able to rupture and imperil the patient.
CT's ability to depict vulnerable plaques has been shown previously, but low sensitivity has been an issue, noted Dr. Harald Seifarth in a study presented at the RSNA 2012 meeting.
"[Coronary CT angiography (CCTA)] can more or less reliably detect noncalcified plaque, depending on the size of the plaques, but differentiation from lipid-rich plaques just based on Hounsfield unit values is not possible because of the relatively large overlap in HU values between plaque categories," Seifarth said. "Recently, however, plaques of a ring-like appearance in CCTA were described and correlated to culprit lesions in CT, as well as yellow plaques in primary angioscopy, and one study correlated them to advanced atherosclerotic lesions in histology."
All of these studies found that the napkin-ring sign, defined as plaque with a hypodense center surrounded by a hyperdense rim, has both high specificity and high positive predictive value for detecting lipid-rich and advanced plaque, he said. However, the sensitivity was very low in all of those studies -- only 25% to 30% -- so the aim of the MGH study was to identify histologic characteristics and morphology in those advanced lesions that predict the delineation of the napkin-ring sign in CCTA.
 |
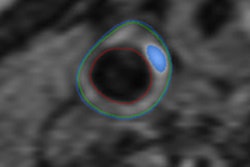
| Above, the napkin-ring sign at 64-detector-row CT. Below, histology of the same vessel shows necrotic/lipid core. Images courtesy of Dr. Harald Seifarth. |
 |
Seifarth and colleagues examined seven human donor hearts using high-resolution CT (Discovery CT750 HD, GE Healthcare). They used a CCTA protocol with 0.625-mm collimation, along with adaptive statistical iterative reconstruction (ASIR, GE).
To correlate between CT and histology, histological slicing and stainings were performed in 1-mm increments along each major coronary artery, Seifarth said. At CCTA, plaques were classified based on the presence or absence of the napkin-ring sign.
At histology, the researchers looked for the presence or absence of a lipid core and microcalcifications, subdivided into sheets of 50 and 100 microns. Quantitative measures included the vessel area, plaque area, area of lipid or necrotic core, and the area of noncore plaque, Seifarth said. The histologic results were coregistered with the CT data and classified according to the modified American Heart Association classification. Two readers, working in consensus, determined the presence or absence of the napkin-ring sign in the CTA studies.
The group coregistered a total of 611 cross sections between the modalities and found 139 (23%) lesions with advanced histology, 33 (24%) of which showed the sign at CCTA. The distribution was such that in early fibroatheroma the group found only a few napkin-ring signs, whereas in those with late atheromas, roughly two-thirds (61%) showed the sign and one-third didn't (38%, p = 0.03), he said.
In addition, the area of the necrotic or lipid core was generally larger in plaques with the sign (median 1.1 mm2 for the sign; 0.5 mm2 for no sign; p = 0.05). Angiogenesis (48% with the sign; 30% without it) and absence of microcalcifications (27% with the sign; 46% without it) tended to be more frequent with the napkin-ring sign, but the difference was not statistically significant (p = 0.06 and p = 0.07).
There was also no statistically significant difference in the presence and extent of intraplaque hemorrhage and the presence of macrophages between plaques with the sign and those without it (all p ≥ 0.27), according to the study team.
Finally, a multivariate analysis showed that necrotic/lipid core area (odds ratio [OR] = 2.1), fibrous/calcified plaque area (OR = 1.7), and total vessel area (OR = 0.9) were independent predictors of the napkin-ring appearance in CCTA (all p < 0.007).
"These three criteria together can explain about 80% of napkin-ring signs that we could actually see," Seifarth said. "So we concluded that atherosclerotic plaques with positive NRS at histology have a certain very distinct appearance: They have a large lipid core, a large plaque area, and a large vessel area, and borderline [statistical significance] was reached for neovascularization and absence of calcifications" for the presence of NRS.
Considering that all of these properties have been previously associated with a high risk of atherosclerotic lesions by either optical coherence tomography or histology, "we can say that the presence of the napkin-ring sign might be a marker for those high-risk plaques and might be also for patients at risk of developing [acute coronary syndrome]," Seifarth said.
Histological features associated with lipid/necrotic core
|
After Seifarth's talk, an audience member commented that visualization of the sign only with larger lesions suggests there are still some spatial resolution challenges.
Seifarth responded that having also looked at the images with filtered back projection reconstruction and the more advanced model-based iterative reconstruction (MBIR, GE) algorithm, it appears that iterative reconstruction makes it easier to distinguish the napkin-ring sign but does not change the findings significantly. Also, because the larger lesions are more clinically relevant, ASIR appears to be seeing the napkin-ring signs that matter, he said.