After more than 1,000 PET cases, Dr. Harry Agress Jr. has come to expect the unexpected. Whether it be handling unforeseen logistical demands, educating referring physicians, or finding unexpected cancer, the nuclear medicine chief at Hackensack University Medical Center (HUMC) in New Jersey has seen his fair share of surprises. Agress described PET's rapid growth in a community hospital at the 2001 Society of Nuclear Medicine meeting in Toronto.
The 600-bed HUMC began PET services in May 1999, performing coincidence detection studies with a gamma camera. The facility couldn't purchase a dedicated scanner until April 2000 because New Jersey forbade the acquisition until then. The center upgraded to dedicated PET in November of that year.
The scanner is located in an outpatient center connected to the hospital, and was paid for by the hospital. By June of this year, HUMC had performed 1,180 PET studies, 480 of which were coincidence detection scans (prior to installation of the dedicated PET scanner). With favorable reimbursement decisions effective in July and expanding clinical applications for PET, scanning volume will soon rise higher, Agress believes.
Implementing PET successfully
Education -- both for yourself and for referring physicians -- is crucial to implementing PET successfully, Agress said. Visits to a successful PET site can help, as well as joining the Academy of Molecular Imaging (formerly the Institute for Clinical PET). Keeping up with journals such as Seminars in Nuclear Medicine, the Journal of Nuclear Medicine, Radiology, Clinical Positron Imaging , and the Journal of Clinical Oncology is also important, he said.
Having relevant PET journal articles and abstracts readily available can aid in the difficult task of educating referring physicians, Agress said.
"When you're about to introduce PET to a group of physicians who are completely used to thinking in terms of CT, MR, and tumor markers, unless they have been well-educated at their own meetings, resistance can be astonishing," he said.
Some recommended articles to have handy include:
- PET Imaging in Oncology, Seminars in Nuclear Medicine, July 2000: Vol. 30:3, pp. 150-185.
- Oncological Applications of FDG PET Imaging, JNM, October 1999, Vol. 40:10, pp. 1706-1715.
- PET in Lung Cancer, JNM, May 1999, Vol. 40:5, pp. 814-820.
- Impact of 18F-FDG PET on Managing Patients with Colorectal Cancer: The Referring Physician’s Perspective, JNM, April 2001, Vol. 42:4, pp. 586-590.
- PET: The Merging of Biology and Imaging into Molecular Imaging; JNM, April 2000, Vol. 41:4, pp. 661-681.
Agress also suggests keeping useful cases to show referring physicians. Microsoft PowerPoint is a great tool for storing these studies and giving quick presentations, he said. With PowerPoint, slides can quickly be changed to tailor the presentation for a particular physician or group.
"It's important to get presentations for grand rounds, tumor boards, subspecialties, etc.," he said. "They will not come running to you in the beginning."
Particularly poignant cases should also be shown to fellow nuclear medicine physicians and radiologists to give feedback on PET vs. CT, he said. In addition, radiologists can become a major referral source, based on the imaging studies they're evaluating.
Logistics
It's easy to underestimate the logistical demands of putting in a PET service, Agress said.
"This is not your father's bone scan," he said. "This is not something you can look at, just bang it out, and go on to the next case. PET is a major time commitment on the part of the physician in charge and the staff."
Demands were also unexpectedly high on the technologists as well as support staff at HUMC's nuclear medicine department, Agress said. To compensate for the increased workloads, Agress was forced to ask administration for raises for the staff. A good relationship with HUMC president and CEO John Ferguson was invaluable during this process, Agress said.
To improve organization, all clinical and insurance forms should be filled out prior to approving and scheduling any PET scans, he said. In addition, Agress believes that PET should be separated from the rest of the nuclear medicine department, at least psychologically. This would include having a separate phone line for PET, as well as a dedicated PET receptionist/coordinator.
By informing administration early on about the staffing requirements for PET and securing support, the department will be well-positioned for expected increases in business.
"You need to be prepared for success at the start," he said. "I highly suggest you overstaff in the beginning, or be ready to take on people when that (increased scan volume) begins."
Correlating images
PET studies should be read along with the CT or MR study that sparked the request for PET, to ensure an accurate evaluation. In addition, the diagnostic report should reflect this consultative approach, correlating findings with that of the CT or MR study, Agress said.
"The impression should take into account as much of the imaging findings as possible, and not just say that, 'This PET scan shows a hot spot in the left rib'," he said. "If there's an abnormality on CT, then say, 'This correlates with the CT findings.' The more you can pull it all together, the more the referring physician will be happy with that."
To reinforce the value of PET to referring physicians and patients, it's crucial to follow up on the patient to confirm diagnosis, he said.
"Confidence and expertise comes mostly from proven cases," he said. "Follow up until you get tissue (findings)."
Clinical dividends
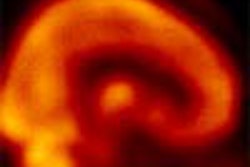
An extensive case experience at HUMC has proven PET's ability to detect cancers missed on CT scans. In one case, an outside CT study of a 68-year-old woman with rectal melanoma (see below) showed a rectal mass, but with no evidence of metastases. A PET study performed two weeks later at HUMC, however, revealed hepatic and pulmonary metastases.
 |
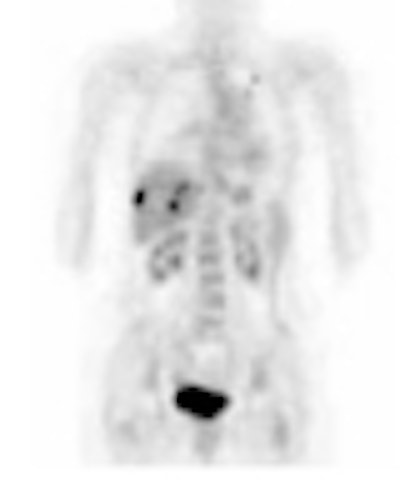
PET yields its share of unexpected malignancies as well. Since November, unexpected second primary cancers were diagnosed in seven patients from PET in areas not related to the original request for the imaging study, Agress said. As such, PET findings should be used to tailor follow-up CT or MR scanning, Agress said.
 |
In addition, PET often determines patient condition to be worse than initially suspected, he said.
"PET tends to upgrade lesions much of the time," he said. "If the oncologist waits for the CT to become positive when they're doing surveillance studies for follow-up, there's a very good chance that they may be too late to detect the earliest recurrence."
In the future, PET may become the preferred imaging modality for surveillance scanning, Agress said, with MR and CT scans used to confirm abnormalities and to provide precise localization for biopsies. To some extent, this change may already be underway.
"I recently had a conversation with an oncologist who had a breast cancer patient with a strong CT contrast allergy on surveillance," he said. "The oncologist requested that the insurance company pay for a noncontrast CT so he could at least see something, and then perform an MRI for the liver. The insurance company said, 'Why don't you just do a PET scan?'"
By Erik L. RidleyAuntMinnie.com staff writer
August 9, 2001
Thinking about starting a PET service in your community? Join Dr. Agress and other expert moderators in our General Discussion Group from Aug. 13-17 for "How to Start a PET Service," a week-long forum covering all aspects of PET.
Related Reading
Reimbursement drives huge growth in PET, August 7, 2001
Focus on PET pays off for CTI as modality booms, August 6, 2001
PET's role in esophageal cancer evolves, August 2, 2001
PET reveals relapse potential for women with eating disorders, July 20, 2001
FDG-PET detects sites of bone, soft tissue infections, July 2, 2001
Triple-detector PET may improve peripheral lesion sensitivity, June 28, 2001
Copyright © 2001 AuntMinnie.com