A study to determine the diagnostic limitations of low-dose, unenhanced CT scans performed for anatomic reference and attenuation correction during PET/CT has found that most discrepancies were due to the lack of intravenous contrast, which obscured liver metastases and lymph node recognition.
In addition, Dr. Marc Gollub and colleagues from Memorial Sloan-Kettering Cancer Center and New York-Presbyterian Hospital/Weill Cornell Medical Center, both in New York City, noted that most missed findings on the unenhanced CT portion of the PET/CT scans were due to technical factors that could be altered.
By documenting the limitations in various organ systems and for various tumor types, the researchers sought to cite the advantages of either PET/CT with intravenous contrast or, if appropriate, suggest the need for limited additional diagnostic contrast-enhanced CT. Details are published in the Journal of Nuclear Medicine (October 2007, Vol. 48:10, pp. 1583-1591).
The team analyzed information for 100 patients from a nine-month period from July 2002 to April 2003. There were 62 males and 38 females, ranging in age from 4 to 83 with an average age of 55.6 years. All PET/CT scans were full-body scans.
Scanning procedures
Within two weeks before or after a PET/CT scan, a diagnostic CT procedure was performed on either a four- or eight-detector-row helical CT scanner (LightSpeed and LightSpeed Ultra, GE Healthcare of Chalfont St. Giles, U.K.) with 5-mm slices.
Oral contrast of 1,000 mL was administered 45 to 60 minutes before scanning. Patients who received oral contrast immediately before PET/CT were given 8 to 16 ounces of additional contrast to fill the stomach. Nonionic intravenous contrast of 150 mL was administered at a rate between 1.5 and 4.0 mL/min, depending on venous access and scan type.
Patient demographics and primary malignancies also were noted. In 85 cases, diagnostic CT scans covered the chest, abdomen, and pelvis, with 10 scans for the chest and abdomen only and five cases in which the abdomen and pelvis were scanned exclusively. Malignancies included 37 cases of lymphoma, 31 patients had colorectal cancer, and 15 scans were for esophageal cancer. There were two cases each for cholangiocarcinoma, lung cancer, neuroblastoma, and soft-tissue sarcoma, and one case each for breast, gallbladder, gastric, hepatocellular, pancreatic, and prostate cancer, as well as unknown primary cancers and myelodysplastic syndrome and melanoma.
One radiologist interpreted the CT portion of the PET/CT scan without knowledge of the PET and diagnostic CT results. Another radiologist compared PET/CT and diagnostic CT images, and classified "true" discrepancies into five categories: intravenous contrast, patient arm-position artifact, lack of enteric contrast, low milliamperage (mA), and quality of lung images.
True discrepancies
Among 194 true discrepancies in which findings were missed by PET/CT, the lack of intravenous contrast was the reason for the discrepancy in 128 cases (66%). Arm-down position artifact was the second most common in 17 cases (9%), followed by quality of lung images in 26 patients (13%), lack of enteric contrast in 15 cases (8%), and low mA with eight patients (4%).
 |
 |
| The diagnostic CT image (top) shows a patient with colorectal cancer with hepatic metastasis in the left hepatic lobe (arrow), but it is not on PET/CT (above). The corresponding PET image (below) confirms metastasis. The study notes that treatment was not changed, as it was seen by PET scan. "Limitations of CT during PET/CT" (Journal of Nuclear Medicine, Vol. 48:10, pp. 1583-1591). Reprinted by permission of SNM. |
 |
The discrepancy due to the lack of intravenous contrast material "most often led to undetected liver metastases or poor lymph node recognition, and most often was apparent in patients who were likely to have liver metastases and undergo PET/CT -- that is, patients with colorectal cancer," the researchers wrote.
In addition, they noted that some metastases could be seen on PET/CT "if a wide window/level was applied to the CT image or if the metastases were large or metabolically active enough to be seen on PET."
Thus, the researchers concluded that if additional research confirms that the intravenous contrast bolus can be given without interfering with CT attenuation mapping or tumor activity assessment, duplicate CT scans should not be performed, in part, to avoid additional radiation and the unnecessary use of time and resources.
Most common issues
The second significant finding was in regard to missed lung findings, due to the occurrence of motion artifact from quiet respiration compared with breath-hold diagnostic CT or the reconstruction kernel used when displaying lung images. CT scanners with more detectors will not overcome motion artifacts from the quiet breathing technique used to match the PET acquisition, the researchers stated.
The third most common reason for discrepancies was the arm-down position of patients for both PET/CT and CT portion. The patient positioning resulted in a beam-hardening artifact, which was most severe in the same horizontal plane in which the arms were resting. More efficient collimator crystals could result in more rapid, arm-up PET as is done in routine diagnostic CT, they stated.
 |
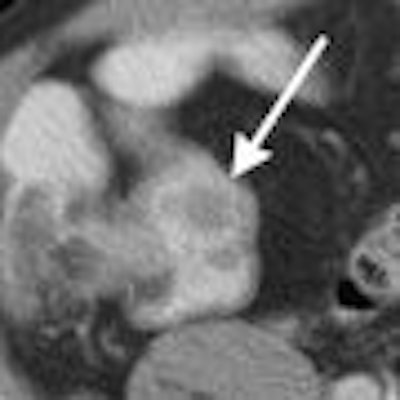
| The image shows a patient with lymphoma and nodules in terminal ileum (arrow). The nodules are not apparent on PET/CT without benefit of oral contrast. The finding is clinically significant, because it could represent extranodal spread of lymphoma. It proved to be Crohn's disease after colonoscopy and surgical removal. "Limitations of CT during PET/CT" (Journal of Nuclear Medicine, Vol. 48:10, pp. 1583-1591). Reprinted by permission of SNM. |
The researchers noted some limitations to the study. Because the patient sample came from a tertiary cancer facility, patients may have more advanced disease than the overall population of patients undergoing PET scans elsewhere.
In addition, they stated that it was "difficult to determine whether the lack of intravenous contrast or beam-hardening artifact (or both) was the cause of the discrepant readings in some cases of obscured liver metastases." A greater number of discrepancies was possibly due to the lack of intravenous contrast.
The researchers also noted the potential for bias with the PET/CT scan reading in a study setting -- as opposed to the reading of diagnostic CT in a clinical setting -- which could produce more accurate readings of PET/CT compared to diagnostic CT.
While additional research would yield a better cost-benefit analysis, the study results suggests that adjustments can be made to better tailor CT when combined with PET, according to the researchers.
They noted that patients with colorectal cancer and other epithelial primary malignancies "will probably need full-body diagnostic scans because about one-half of discrepancies occurred in sites outside of the liver, including small peritoneal implants and small lung nodules."
And, for patients who need additional diagnostic CT scanning, the procedures could be limited to the chest and abdomen as "little additional information seems to be gained from the pelvic portion of diagnostic CT scans," the researchers stated.
By Wayne Forrest
AuntMinnie.com staff writer
November 22, 2007
Related Reading
PET/CT shows great sensitivity, concordance with soft-tissue sarcoma, August 23, 2007
Dual-phase PET/CT useful in lung nodule assessment, April 4, 2007
PET useful for staging pediatric bone sarcomas, February 7, 2003
PET/CT, whole-body MRI each has merits in metastatic breast disease, May 29, 2007
Whole-body FDG-PET of little use in breast cancer staging, November 26, 2006
Copyright © 2007 AuntMinnie.com

















