Simultaneous PET/MRI performs better than PET and MRI performed separately for the detection of FDG-avid pulmonary nodules and lesions at least 0.5 cm in size. However, it has problems with non-FDG-avid nodules and smaller lesions, researchers report in the September issue of Radiology.
Simultaneous PET/MRI identified 86 (96%) of 90 FDG-avid pulmonary nodules and 78 (89%) of 88 nodules with a diameter of 0.5 cm or larger, in the study from NYU Langone Medical Center in New York City.
PET/MRI was less proficient in finding lesions smaller than 0.5 cm, achieving a sensitivity of only 38% (19 of 50 nodules), and it had a sensitivity of only 23% (11 of 48) for nodules that were not FDG-avid (Radiology, Vol. 268:3, pp. 874-881).
Debate over pulmonary nodules
"The recent introduction of whole-body PET/MR imaging systems has reignited the debate regarding the ability of MR imaging and PET/MR imaging to depict pulmonary nodules," wrote lead author Dr. Hersh Chandarana and colleagues from the department of radiology.
As the authors noted, past research has suggested that whole-body combined PET/MRI should be able to enhance the assessment of malignant tumors, given the functional data provided by MRI and the activity recorded by PET. "However, one of the concerns of replacing the CT portion of PET/CT with MRI is the ability of MRI to depict lung nodules," they wrote.
In this study, all patients with tumors who were undergoing clinically indicated routine FDG-PET/CT at the medical center were recruited to undergo PET/MRI following PET/CT. An FDG tracer was injected prior to PET/CT, and PET/MR data were acquired afterward.
Between August 2012 and October 2012, 886 patients underwent whole-body oncologic PET/CT at the medical center. Of those patients, 67 received PET/MRI scans following PET/CT. The researchers excluded 35 patients who did not have their thorax imaged.
The remaining 32 patients consisted of 23 women and nine men, who had a mean age of 62.3 years (range, 39 to 79 years). The patients were imaged for a variety of cancers, with breast (10 cases), lung (eight), and ovarian cancer (four) among the most common afflictions.
All patients received 15 mCi of F-18 FDG intravenously prior to PET/CT (Biograph mCT, Siemens Healthcare). PET data were acquired at two- to three-minute scan times per bed position, depending on the patient's weight and uptake time.
PET/MR images were acquired simultaneously (Biograph mMR, Siemens) approximately 120 minutes after the PET/CT exams using the leftover FDG from the earlier injection. The time between FDG injection and PET/MRI scans ranged from 145 to 175 minutes.
PET/MRI sensitivity
PET/CT, which served as the reference for the study, found a total of 69 nodules in 19 of the 32 patients. There were 45 FDG-avid nodules in 13 patients, while 24 nodules demonstrated no FDG-avid activity.
PET identified all 13 subjects with FDG-avid nodules and achieved a sensitivity of 62% (85 of 138) for all nodules and a sensitivity of 94% (85 of 90) for FDG-avid nodules. PET was unable to detect any nodules that were not FDG-avid. (Because the two readers demonstrated substantial agreement in nodule detection for PET and PET/MRI, sensitivity analysis used data from both readers together in one overall analysis, the authors noted.)
PET/MRI identified all 19 patients with nodules and the 13 patients with FDG-avid nodules. Sensitivity for PET/MRI was 70% (97 of 138) for all nodules and 96% (86 of 90) for FDG-avid nodules. The hybrid modality's sensitivity for non-FDG-avid nodules was 23% (11 of 48).
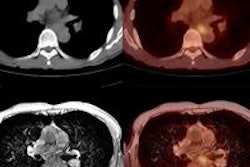
 PET/MRI of a 63-year-old man with a history of lung cancer who underwent diagnostic PET/CT to assess tumor burden. Image shows a left upper lobe lesion (large arrow). A right upper lobe lesion was also found due to FDG avidity. Image courtesy of Radiology.
PET/MRI of a 63-year-old man with a history of lung cancer who underwent diagnostic PET/CT to assess tumor burden. Image shows a left upper lobe lesion (large arrow). A right upper lobe lesion was also found due to FDG avidity. Image courtesy of Radiology.All 13 subjects with FDG-avid nodules were identified by MRI alone. Sensitivity was 62% (43 of 69) for all nodules, 82% (36 of 44) for nodules with a diameter of at least 0.5 cm, and 80% (36 of 45) for FDG-avid nodules. Seven (29%) of the 24 non-FDG-avid nodules and seven (28%) of 25 nodules smaller than 0.5 cm in diameter were detected.
PET/MRI outperformed MRI alone for all FDG-avid nodules, with a sensitivity of 96% versus 80%, regardless of nodule size, according to the authors.
Both readers in the study missed two FDG-avid nodules measuring 0.5 cm and 0.2 cm in one patient, they noted.
While the study showed that simultaneous PET/MRI has high sensitivity in the detection of FDG-avid nodules and nodules at least 0.5 cm in size, the combination "has limited sensitivity in the detection of small non-FDG-avid nodules," they concluded. "The clinical importance of these missed nodules is unclear and needs further investigation."
Study disclosures
One study author is employed by Siemens, which provided research support in the form of PET/MRI workflow and protocols. The other authors, who are not employed by Siemens, had full control of the data, according to the study.