Hybrid SPECT/CT can promptly and accurately find the source of gastrointestinal (GI) bleeding and improve treatment of the condition, according to a study presented at the American Roentgen Ray Society (ARRS) annual meeting in San Diego.
Planar technetium-99m-labeled red blood cell (TRBC) scintigraphy is sensitive for detecting acute bleeding, but it's not always accurate in localizing the bleeding source, noted lead author and presenter Dr. Ajit Goenka, from the Cleveland Clinic, and colleagues.
Therefore, the purpose of the current study was to assess whether fusion imaging with hybrid SPECT/CT could improve localization of the bleeding source in patients with equivocal planar TRBC scintigraphy.
Goenka's group retrospectively reviewed TRBC studies performed between January 2009 and August 2013. They identified 29 patients (14 men, 15 women; mean age, 64 years) who had a concurrent hybrid SPECT/CT scan to evaluate equivocal TRBC activity on planar scintigraphy.
All scans included continuous, dynamic planar acquisition for 60 minutes, followed by immediate SPECT/CT. The average additional time required for SPECT/CT was 20 minutes (range, 13-31 minutes), and mean dose-length product was 139.4 mGy-cm (range, 80-300 mGy-cm).
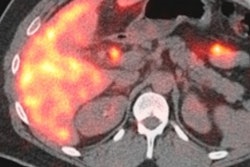
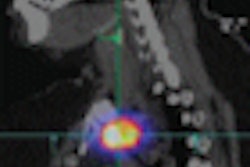
The SPECT/CT findings were reviewed in a blinded manner in combination with planar scintigraphy. The bleeding source was identified on SPECT/CT according to the most intense intraluminal TRBC activity in the gastrointestinal tract on the coregistered images.
For nine patients (31%), SPECT/CT found that scintigraphic TRBC activity was due to nongastrointestinal causes, such as splenosis, a herniated urinary bladder, or focal liver lesions.
In the remaining 20 patients (69%), SPECT/CT localized scintigraphic TRBC activity within the gastrointestinal tract. In 18 of these patients, the bleeding source was subsequently confirmed at surgery (four), colonoscopy (six), double balloon enteroscopy (six), and invasive angiography (two). The two patients for whom the bleeding source wasn't determined were excluded from the analysis.
For the 18 patients, SPECT/CT did correctly identify the source of bleeding, achieving an accuracy of 100%. The causes were diverticulosis (seven), small intestinal (five) and colonic (one) vascular anomalies, small intestinal anastomotic bleeding (one), recurrent duodenal ulceration (two), and ulceration related to gastric bypass (two).
SPECT/CT fusion imaging correctly localized the GI bleeding source with minimal additional time and radiation exposure, Goenka and colleagues concluded. "Hybrid SPECT/CT also reduces ambiguities in interpretation of planar scintigraphy by identifying the confounding, non-GI sources of TRBC activity owing to optimal demonstration of regional anatomy," they wrote.
Based on the performance of SPECT/CT in the study, the researchers are working to make it part of routine practice at the Cleveland Clinic.