European researchers have set the groundwork for what they believe is a feasible way to achieve optimal image quality in PET/MRI scans: balancing lower radiotracer dose with prolonged PET image acquisition time to match the longer duration needed for MR image acquisition.
In the study, published in the August issue of the Journal of Nuclear Medicine, the researchers used a specially designed phantom and continually reduced FDG activity by 50% while simultaneously lengthening image acquisition time from two minutes (when FDG activity was 100%) to 16 minutes (when FDG activity was 12.5%).
Although the exams occurred under "idealized" experimental conditions, the results "identify a further advantage of integrated PET/MR hybrid imaging in the context of reducing patient radiation exposure," wrote lead author Mark Oehmigen, from the University of Erlangen-Nuremberg in Germany, and colleagues.
"This experiment may serve as a basis for further clinical PET/MR studies using reduced radiotracer dose as compared with conventional PET/CT studies," they wrote (JNM, August 2014, Vol. 55:8, pp. 1361-1367).
The downside of PET/CT
The introduction of PET/CT revolutionized medical imaging by uniting metabolic and anatomic information in a single exam. But the downside has been that patients are being scanned with two radiation-bearing modalities rather than one.
One of the major benefits of PET/MRI is the reduction in radiation exposure compared with standard PET/CT scans. Because PET image quality is a balance of acquisition time and radiotracer activity, Oehmigen and colleagues theorized that radiation exposure could be reduced even more by lowering radiotracer doses and coordinating PET image acquisition time with the longer time needed for MRI.
For example, in conventional PET/CT hybrid imaging, PET data acquisition typically lasts two to three minutes per bed position. Meanwhile, PET data acquisition in whole-body PET/MRI generally ranges from five to 10 minutes per bed position, and MRI examinations with multicontrast protocols may take as long as 20 minutes depending on the clinical application.
"Therefore, adapting and increasing the PET data acquisition times to the prolonged MR examinations may allow for decreasing the injected patient radiotracer activity, compared with clinical PET/CT protocols," the authors wrote.
Customized phantom
The researchers used a PET phantom that met National Electrical Manufacturers Association (NEMA) specifications and mimicked the shape of the upper human body. The device was made of acrylic glass, had an inner volume of approximately 9.5 L, and contained a spongy material to resemble the attenuating properties of human lung tissue.
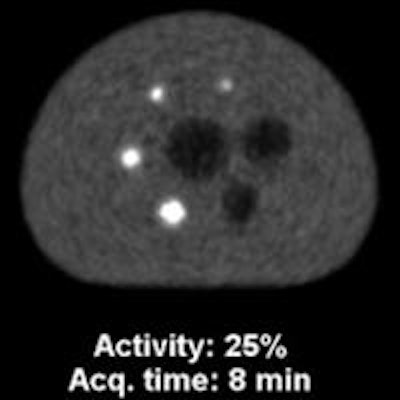
Inside the phantom, there were six hollow glass spheres of different diameters: Four small spheres contained FDG to represent "hot," or malignant, lesions, and two larger spheres contained nonradioactive water to represent "cold," or benign, lesions.
All phantom images and measurements were performed on an integrated whole-body PET/MRI hybrid system (Biograph mMR, Siemens Healthcare), which allows for simultaneous PET and MR imaging.
To further evaluate PET image quality, Oehmigen and colleagues assessed contrast recovery, background variability, and signal-to-noise ratio under the varying radiotracer activity and timing conditions.
PET data were acquired at two-, four-, eight-, and 16-minute time points to coincide with 50% reductions in FDG activity, which began at 100% and dropped to 50%, 25%, and 12.5% at the second, third, and fourth image acquisition time points, respectively. To confirm the results, the entire experimental protocol was repeated three times.
For qualitative image analysis, five experienced readers were asked to rate image quality and group images from best to worst based on their visual observation. Sixteen images representing the various acquisitions and FDG activity were randomized. If there were no detectable differences, the readers were asked to place those images in the same group of comparable image quality.
Consistent results
After decreasing FDG radiotracer activity and lengthening image acquisition times, Oehmigen and colleagues found very little noticeable difference among the phantom images at the different time points.
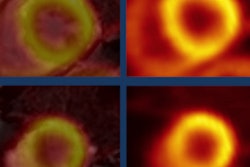
 PET image quality as FDG activity decreases over time and data acquisition time increases. Above and below, radiotracer activity was reduced by half (100%, 50%, 25%, and 12.5%), while data acquisition times doubled (two, four, eight, and 16 minutes). Differences in overall quality were hardly perceivable. Images courtesy of JNM.
PET image quality as FDG activity decreases over time and data acquisition time increases. Above and below, radiotracer activity was reduced by half (100%, 50%, 25%, and 12.5%), while data acquisition times doubled (two, four, eight, and 16 minutes). Differences in overall quality were hardly perceivable. Images courtesy of JNM.
Contrast recovery, background variability, and signal-to-noise ratio remained stable over the three FDG half-life periods, according to the authors.
Contrast recovery fluctuation was small, with a mean variation of 2%, compared with the reference point of 100% FDG activity and two-minute image acquisition time. In addition, only small differences were observed in background variability; mean variation over the three half-life periods was 4%.
As for the signal-to-noise ratio, the four "hot" spheres showed only minor variations over the three half-life periods. The largest variation was seen in the smallest sphere, which had a diameter of 10 mm; there was 15% variation at the end of the third half-life, compared with the 100% tracer activity, two-minute reference.
"Otherwise, the signal-to-noise ratio remained nearly constant, with a variation of 5%," the authors wrote.
As one might expect, all five readers rated the image from 100% FDG activity and a 16-minute acquisition time as the best among the group. They also rated the 12.5% activity, two-minute acquisition image as having the worst quality. Otherwise, the five readers generally agreed that decreasing FDG activity while increasing acquisition time resulted in comparable image quality.
Maintaining PET image quality at "lower injected tracer activity by increasing the acquisition time is viable," Oehmigen and colleagues concluded, and this approach "may lead to reduced radioactive tracer dose."
However, they cautioned that the results were achieved under controlled circumstances.
"Before conclusions for a clinical application of tracer activity reduction can be drawn, further factors such as biodistribution of the tracer in different lesions and background over time ... need to be considered that ultimately may influence lesion detectability in vivo," they wrote.