Add SPECT to the list of imaging modalities that can help physicians distinguish between post-traumatic stress disorder (PTSD) and traumatic brain injury (TBI), potentially leading to more appropriate treatment for military veterans.
In a new study published online April 23 in Brain Imaging and Behavior, SPECT clearly showed perfusion differences in the brain's default mode network that could enable radiologists to distinguish TBI from PTSD, according to the researchers.
Understanding whether a person has PTSD, TBI, or both can significantly change the management of their disorder, said lead author Dr. Cyrus Raji, PhD, a radiology resident at the University of California, Los Angeles (UCLA).

"It is hard to tell clinically sometimes which disorder is the more dominant disorder and which the patient has," Raji said. "It can then be harder to plan treatment. Knowing who has PTSD or TBI or both is actionable information."
For example, treatment for PTSD can be "harmful or, at best, not helpful in the case of TBI," the authors wrote. They cited previous studies that found that exposure therapy, cognitive processing therapy, and trauma-focused cognitive behavioral therapy can help with PTSD, but "there is no evidence to suggest that [these treatments] would be helpful for those with mild TBI who are misdiagnosed as having PTSD."
This study is not the first time Raji and colleagues have explored the value of SPECT for TBI. A 2014 study showed that SPECT outperformed "both CT and MRI in both acute and chronic imaging of TBI, particularly mild TBI." SPECT also had close to 100% negative predictive value, they wrote (PLOS One, March 19, 2014).
SPECT could be an "important second test in settings where CT or MRI are negative after a closed head injury with postinjury neurological or psychiatric symptoms," they concluded in the PLOS One article.
Afflicted veterans
In the current study, the researchers analyzed 196 peacetime or combat veterans from the Army, Navy, Marines, and Air Force who had a diagnosis of PTSD, TBI, or both. There were 115 cases of TBI, 36 cases of PTSD, and 45 veterans with both disorders.
Each participant received two SPECT scans. A baseline exam was given at rest, while a second scan was performed as the veterans were engaged in a concentration task. The purpose of the concentration scan was to visualize brain activation when subjects were given certain tasks.
"In looking at brain activation patterns, we can uncover information that would be helpful in different types of disorders," Raji said.
The researchers honed in on the brain's default mode network regions, including the bilateral angular gyrus, anterior and posterior cingulate gyri, precuneus, inferior orbital frontal cortex, superior parietal lobe, hippocampus, and parahippocampal gyrus.
Abnormal findings in the default mode network are an indication of neurological and psychiatric disorders. For example, hyperperfusion in the default mode network suggests PTSD, while hypoperfusion is a sign of TBI.
"By further elucidating the correlation between increased perfusion in default mode network structures in PTSD and decreased perfusion in TBI, clinicians may be able to more reliably diagnose PTSD from TBI," Raji and colleagues wrote.
ROC analysis
The researchers used receiver operator characteristics (ROC) analysis to determine sensitivity, specificity, and accuracy.
The ROC data showed that quantitative SPECT had an accuracy range of 87% to 94% for differentiating between veterans with PTSD and those with TBI. The scans were able to distinguish veterans with TBI from those with both PTSD and TBI with an accuracy of 79% to 83%. Meanwhile, accuracy was 85% to 92% for distinguishing those with PTSD from those with both conditions.
| Performance of SPECT default mode network scans | |||||
| Measure | Baseline scan | Concentration scan | Baseline-concentration* | ||
| Separating PTSD from TBI | |||||
| Sensitivity | 92% | 85% | 85% | ||
| Specificity | 85% | 83% | 80% | ||
| Accuracy | 94% | 89% | 87% | ||
| Separating PTSD/TBI from TBI | |||||
| Sensitivity | 85% | 80% | 82% | ||
| Specificity | 81% | 65% | 69% | ||
| Accuracy | 83% | 79% | 81% | ||
| Separating PTSD/TBI from PTSD | |||||
| Sensitivity | 87% | 91% | 84% | ||
| Specificity | 83% | 76% | 64% | ||
| Accuracy | 92% | 88% | 85% | ||
"The data suggests that ... the default mode network is implicated in both PTSD and TBI contributing to the similarity in symptoms," the authors concluded. "However, the pathophysiologies of the diseases are different in the way they affect perfusion of the default mode network. SPECT may therefore allow clinicians to differentially diagnose PTSD and TBI."
"What we are finding is that more and more of the psychological manifestations that we see in different disorders have underlying brain changes," Raji said. "In traumatic brain injury, there is a lot of physical damage to the brain, either from blast injuries or direct impact."
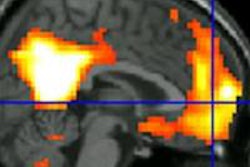
 SPECT images show the differences between a healthy person and veterans with PTSD, TBI, or both disorders. The veteran with PTSD shows increased perfusion, particularly in the frontal lobes. The veteran with TBI shows decreased perfusion throughout the same brain region. A veteran with both PTSD and TBI has perfusion that is intermediate -- lower than in the person with PTSD, but higher than in the individual with TBI. Image courtesy of Dr. Cyrus Raji.
SPECT images show the differences between a healthy person and veterans with PTSD, TBI, or both disorders. The veteran with PTSD shows increased perfusion, particularly in the frontal lobes. The veteran with TBI shows decreased perfusion throughout the same brain region. A veteran with both PTSD and TBI has perfusion that is intermediate -- lower than in the person with PTSD, but higher than in the individual with TBI. Image courtesy of Dr. Cyrus Raji.The big picture
Perhaps most importantly, the study's affirmation of SPECT imaging for PTSD and TBI contributes to the broad clinical strategy of gathering as much information as possible about the disorders from a variety of imaging modalities, including diffusion-tensor MRI (DTI).
"DTI will show specific fibers in white matter that are abnormal, and SPECT will show perfusion or blood flow changes," Raji said. "We are dealing with an ecosystem of different brain imaging modalities that are giving different forms of information, all of which are useful by themselves. I think in the future there should be studies that combine all of these modalities together."
This confluence of information from different modalities regarding PTSD and TBI could follow the same strategy as what researchers are doing to unlock the mysteries of Alzheimer's disease and other neurological conditions.
"What we are finding is that more and more of the psychological manifestations that we see in different disorders have underlying brain changes," Raji added. "In traumatic brain injury, there is a lot of physical damage to the brain, either from blast injuries or direct impact."
Raji and colleagues already plan to expand this study to investigate TBI in the civilian population, with a goal of collecting SPECT data from more 20,000 patients.
"We expect that once that data is published, we will be able to develop knowledge on how perfusion imaging and blood flow imaging with SPECT can be useful in a larger, more general population," he said.
The findings may be most helpful for patients with mild TBI who do not exhibit classic or blatant symptoms of the injury. In those cases, accurate imaging is crucial, Raji added, "because if the person has a mild traumatic brain injury, that can often be missed."