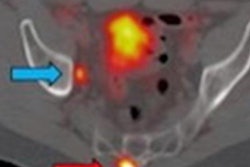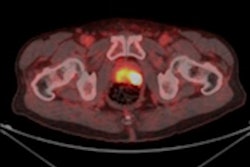
Researchers from the University of California, Los Angeles (UCLA) say it is time to reconsider guidelines in favor of broader use of gallium-68 (Ga-68) prostate-specific membrane antigen-11 (PSMA-11) PET/CT to detect bone metastases in prostate cancer patients, based on findings in their study published September 20 in the Journal of Nuclear Medicine.
The recommendation comes after they "surprisingly" found that approximately 18% of patients with serum prostate-specific antigen (PSA) levels of less than 5 ng/mL had PSMA-positive lesions suspicious for bone metastases. They also observed a higher-than-expected incidence of PSMA-positive lesions in prostate cancer patients with serum PSA levels from 5-10 ng/mL to 10-20 ng/mL.
"Therefore, current guidelines for bone assessments in prostate cancer patients should be revisited as Ga-68 PSMA-11 PET/CT may provide additional information for accurate bone staging at low-serum PSA levels," wrote lead author Dr. Kelsey Lynn Pomykala and colleagues from UCLA's David Geffen School of Medicine.
While the efficacy of Ga-68 PSMA-11 PET/CT to detect bone metastases is well-known, some questions remain as to whether bone lesion incidence varies based on initial staging, biochemical recurrence, or restaging of confirmed metastatic disease. However, scant data are available on the relationship among serum PSA levels, risk scores under National Comprehensive Cancer Network (NCCN) criteria, and other potential biomarkers, such as the Gleason score and bone involvement.
"This information is relevant, as Ga-68 PSMA-11 imaging can have a profound impact on patient management and may inform about necessary adaptations of current guidelines," the authors noted.
To shed more light on the topic, the researchers retrospectively looked at 388 patients with confirmed prostate cancer, all of whom underwent whole-body Ga-68 PSMA-11 PET/CT scans (Biograph 64 TruePoint or 2010 Biograph mCT 64, Siemens Healthineers) for primary staging, biochemical recurrence, or restaging from September 2017 to May 2018. Subjects received a median of 196.1 MBq (5.3 mCi) of Ga-68 PSMA-11, with a median tracer uptake period of 60 minutes.
The images detected bone metastases in 12 (13%) of 93 patients who underwent initial staging; 44 (20%) of 225 patients with biochemical recurrence; and 49 (70%) of 70 restaging patients. As expected, the incidence of bone metastases increased concurrently with rising serum PSA levels.
"Surprisingly, 38 of 216 patients (17.6%) with serum PSA levels of less than 5.0 ng/mL were found to have PSMA-positive lesions suspicious for bone metastases," the authors wrote.
| Incidence of bone metastases on Ga-68-PSMA-11 PET/CT by PSA level | ||||
| Serum PSA levels | < 5 ng/mL | 5-10 ng/mL | 10-20 ng/mL | > 20 ng/mL |
| Incidence rate | 17.6% | 34.4% | 40.8% | 41.4% |
In addition, initial NCCN risk scores were not significantly associated with presence of PSMA-positive bone lesions. The result was "likely due to the long time interval between initial diagnosis and the PET/CT study (median 161 months)," the authors suggested.
Not only do the results suggest a reconsideration of Ga-68 PSMA-11 PET/CT for metastatic bone staging, Pomykala and colleagues wrote, but the study also "demonstrates the importance of initiating a prospective direct comparison between conventional imaging (bone scan, CT, or whole-body MRI, which has replaced bone scans in some institutions) and Ga-68 PSMA-11 PET/CT imaging for bone metastasis staging, and suggests necessary adaptions of bone imaging guidelines in prostate cancer."