Human papilloma virus/ Laryngotracheal papillomatosis
- Clinical:HPV is a DNA virus that typically invovles the larynx [2]. Infection typically occurs at birth due to exposure to HPV in the birth canal- usually with HPV 6 or HPV 11 [1,3]. Involvement of the trachea and proximal bronchi occurs in only 5% of patients [2]. Pulmonary involvement occurs in less than 1% of cases [2] and is felt to be secondary to aerial dissemination, possibly related to recurrent laser treatment or tracheostomy [3]. Most cases occur in childhood with an average of 10 years after the intial diagnosis of laryngeal papillomatosis [3]. The overall prognosis is poor [3]. Patients with tracheobronchial papillomatosis are also at an increased riskfor squamous metaplasia and development of squamous cell carcinoma [3]. This risk is more frequently associated with HPV 11 and 16, but can also be seen with HPV 6 [3].
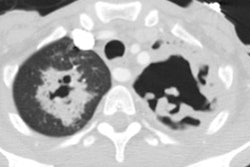
The characteristic finding on CXR of pulmonary parenchymal involvement is scattered multiple thin-walled cysts and nodules- typically in the posterior portions of the lungs [1,2]. The cysts are usually round or irregular in shape and less than 5 cm in diameter [1]. The walls are usually smooth, but asymmetric and measure 2-3 mm in thickness [1]. Nodules measuring less than 3 cm with lobulated margins can also be seen [1].
REFERENCES:
(1) Radiology 2011; Franquet T. Imaging of pulmonary viral pneumonia. 260: 18-39
(2) AJR 1985; Kramer SS, et al. Pulmonary manifestations of juvenile laryngotracheal papillomatosis. 144: 687-694
(3) Radiographics 2001; Raven CE, et al. Image interpretation session:2000. 21: 267-287